

Ticagrelor Added to Aspirin in Acute Nonsevere Ischemic Stroke or Transient Ischemic Attack of Atherosclerotic Origin
- PMID: 33198608
- PMCID: PMC7678660
- DOI: 10.1161/STROKEAHA.120.032239
Ticagrelor Added to Aspirin in Acute Nonsevere Ischemic Stroke or Transient Ischemic Attack of Atherosclerotic Origin
Abstract
Background and purpose: Among patients with a transient ischemic attack or minor ischemic strokes, those with ipsilateral atherosclerotic stenosis of cervicocranial vasculature have the highest risk of recurrent vascular events.
Methods: In the double-blind THALES (The Acute Stroke or Transient Ischemic Attack Treated With Ticagrelor and ASA for Prevention of Stroke and Death) trial, we randomized patients with a noncardioembolic, nonsevere ischemic stroke, or high-risk transient ischemic attack to ticagrelor (180 mg loading dose on day 1 followed by 90 mg twice daily for days 2-30) or placebo added to aspirin (300-325 mg on day 1 followed by 75-100 mg daily for days 2-30) within 24 hours of symptom onset. The present paper reports a prespecified analysis in patients with and without ipsilateral, potentially causal atherosclerotic stenosis ≥30% of cervicocranial vasculature. The primary end point was time to the occurrence of stroke or death within 30 days.
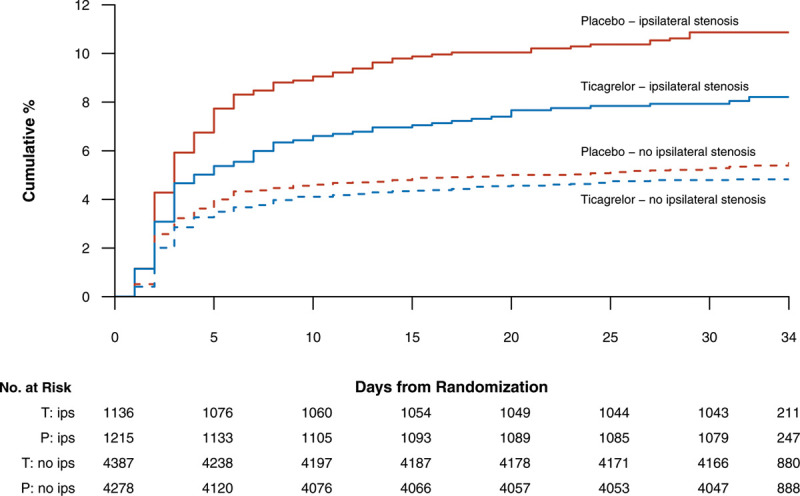
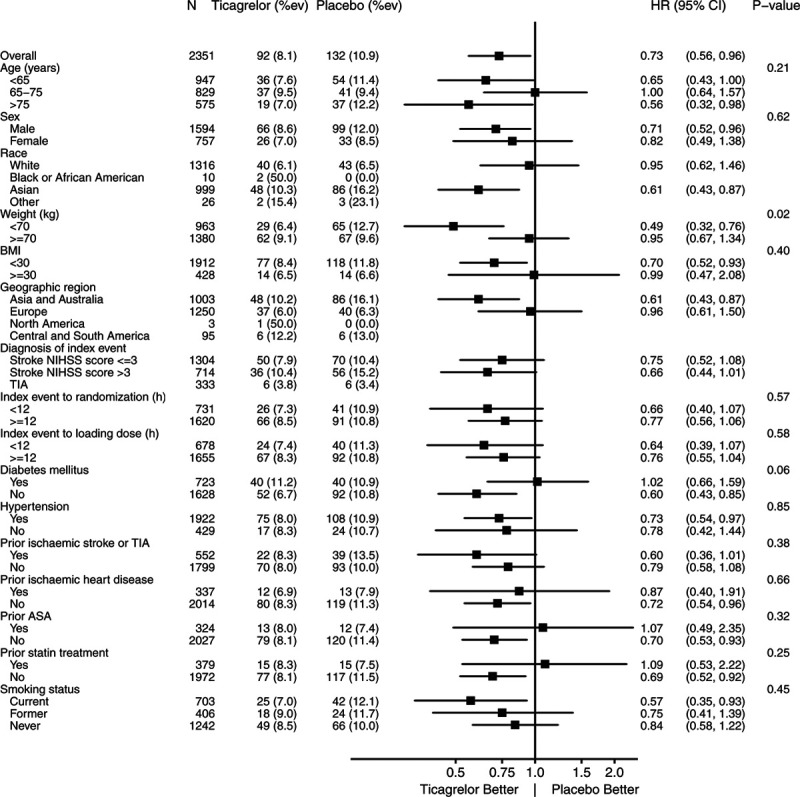
Results: Of 11 016 randomized patients, 2351 (21.3%) patients had an ipsilateral atherosclerotic stenosis. After 30 days, a primary end point occurred in 92/1136 (8.1%) patients with ipsilateral stenosis randomized to ticagrelor and in 132/1215 (10.9%) randomized to placebo (hazard ratio 0.73 [95% CI, 0.56-0.96], P=0.023) resulting in a number needed to treat of 34 (95% CI, 19-171). In patients without ipsilateral stenosis, the corresponding event rate was 211/4387 (4.8%) and 230/4278 (5.4%), respectively (hazard ratio, 0.89 [95% CI, 0.74-1.08]; P=0.23, Pinteraction=0.245). Severe bleeding occurred in 4 (0.4%) and 3 (0.2%) patients with ipsilateral atherosclerotic stenosis on ticagrelor and on placebo, respectively (P=NS), and in 24 (0.5%) and 4 (0.1%), respectively, in 8665 patients without ipsilateral stenosis (hazard ratio=5.87 [95% CI, 2.04-16.9], P=0.001).
Conclusions: In this exploratory analysis comparing ticagrelor added to aspirin to aspirin alone, we found no treatment by ipsilateral atherosclerosis stenosis subgroup interaction but did identify a higher absolute risk and a greater absolute risk reduction of stroke or death at 30 days in patients with ipsilateral atherosclerosis stenosis than in those without. In this easily identified population, ticagrelor added to aspirin provided a clinically meaningful benefit with a number needed to treat of 34 (95% CI, 19-171). Registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT03354429.
Keywords: aspirin; atherosclerosis; death; population; stroke; ticagrelor; transient ischemic attack.
Conflict of interest statement
Dr Johnston has received institutional research support from AstraZeneca and drug/placebo from Sanofi for an National Institutes of Health (NIH)-sponsored trial. Dr Amarenco reports receipt of research grant support from Pfizer, Sanofi, Bristol-Myers-Squibb, Merck, AstraZeneca, Boston Scientific, and from the French government, and consulting fees from Pfizer, BMS, Merck, Boehringer Ingelheim, AstraZeneca, Bayer, Daiichi Sankyo, Edwards, Boston Scientific, Kowa, GSK, Fibrogen, Amgen, Shing Poon, Gilead, and lecture fees from Bayer, St-Jude Medical, Amgen, Pfizer, Sanofi. Dr Evans is a statistical consultant to AstraZeneca. Drs Denison, Himmelmann, Knutsson, and Ladenvall are employees of AstraZeneca. Dr James has received institutional research grants from Astra Zeneca, The Medicines Company, Bayer, and Jansen. Dr Molina has received honoraria for participation in clinical trials, contribution to advisory boards, or oral presentations from AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, Bristol-Myers-, Covidien, Cerevast, and Brainsgate. Dr Wang has received research grants from Sanofi, AstraZeneca and Amgen, and honoraria for participation to advisory board from Sanofi.
Figures
References
-
- Sirimarco G, Lavallée PC, Labreuche J, Meseguer E, Cabrejo L, Guidoux C, Klein IF, Olivot JM, Abboud H, Adraï V, et al. Overlap of diseases underlying ischemic stroke: the ASCOD phenotyping. Stroke. 2013;44:2427–2433. doi: 10.1161/STROKEAHA.113.001363 - PubMed
-
- Amarenco P, Lavallee PC, Labreuche J, Albers GW, Bornstein NM, Canhao P, Caplan LR, Donnan GA, Ferro JM, Hennerici MG, et al. One-year risk of stroke after transient ischemic attack or minor ischemic stroke. N Engl J Med. 2016;374:1533–1542. doi: 10.1056/NEJMoa1412981 - PubMed
-
- Amarenco P, Albers GW, Denison H, Easton JD, Evans SR, Held P, Hill MD, Jonasson J, Kasner SE, Ladenvall P, et al. Ticagrelor versus aspirin in acute stroke or transient ischemic attack of atherosclerotic origin. Lancet Neurol. 2017;16:301–310. - PubMed
-
- Johnston SC, Amarenco P, Denison H, Evans SR, Himmelmann A, James S, Knutsson M, Ladenvall P, Molina CA, Wang Y. Ticagrelor and aspirin versus aspirin in patients with acute ischemic stroke. N Engl J Med. 2020;383:207–217.
-
- Johnston SC, Amarenco P, Denison H, Evans SR, Himmelmann A, James S, Knutsson M, Ladenvall P, Molina CA, Wang Y; THALES Investigators. The acute stroke or transient ischemic attack treated with ticagrelor and aspirin for prevention of stroke and death (THALES) trial: rationale and design. Int J Stroke. 2019;14:745–751. doi: 10.1177/1747493019830307 - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
