

Cerebrovascular Disease Progression in Patients With ACTA2 Arg179 Pathogenic Variants
- PMID: 33199432
- PMCID: PMC7905785
- DOI: 10.1212/WNL.0000000000011210
Cerebrovascular Disease Progression in Patients With ACTA2 Arg179 Pathogenic Variants
Abstract
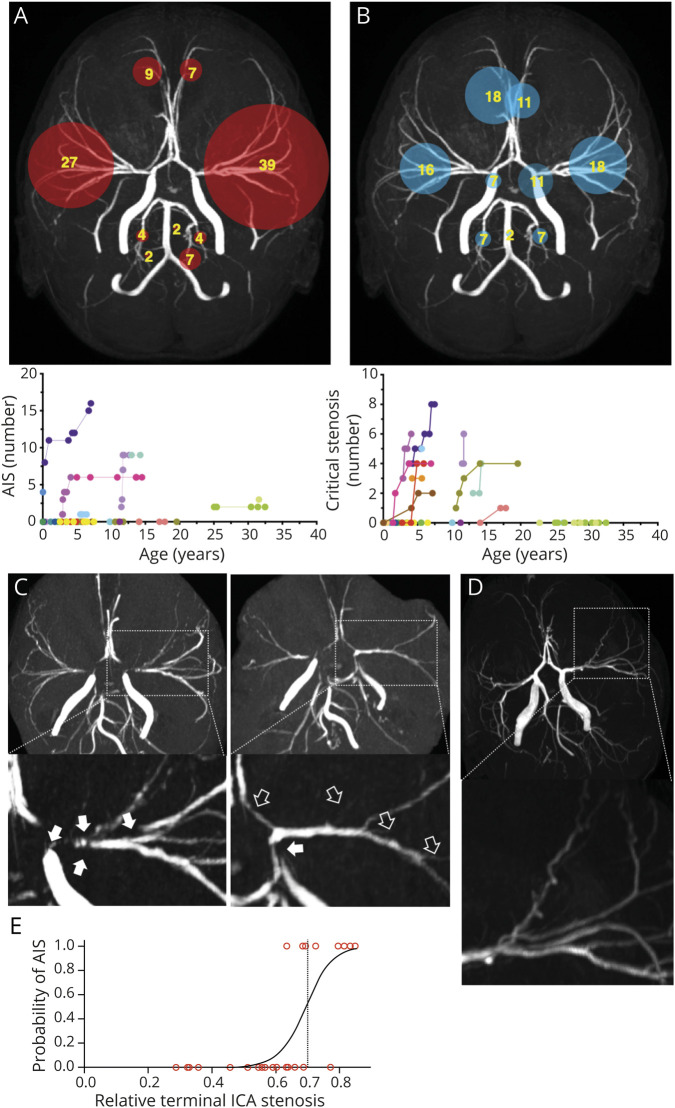
Objective: To establish progression of imaging biomarkers of stroke, arterial steno-occlusive disease, and white matter injury in patients with smooth muscle dysfunction syndrome caused by mutations in the ACTA2 gene, we analyzed 113 cerebral MRI scans from a retrospective cohort of 27 patients with ACTA2 Arg179 pathogenic variants.
Methods: Systematic quantifications of arterial ischemic strokes and white matter lesions were performed on baseline and follow-up scans using planimetric methods. Critical stenosis and arterial vessel diameters were quantified applying manual and semiautomated methods to cerebral magnetic resonance angiograms. We then assessed correlations between arterial abnormalities and parenchymal injury.
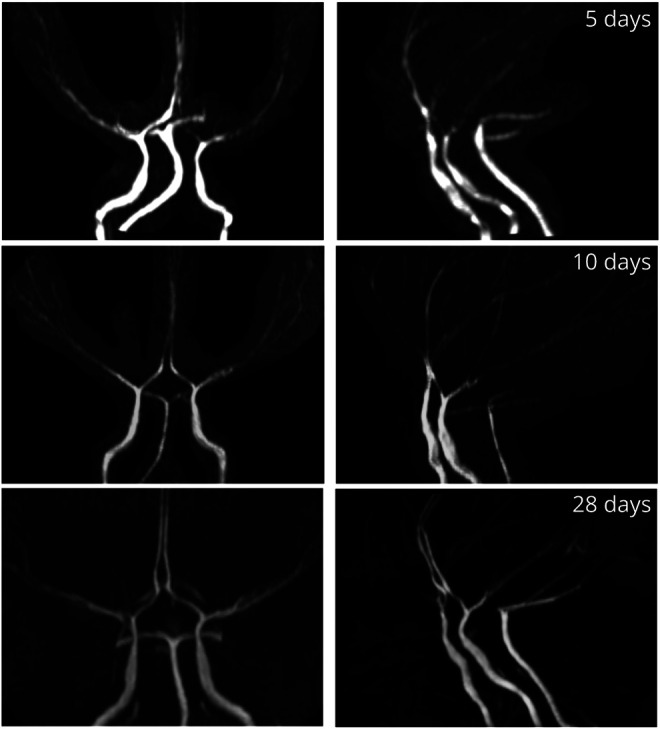
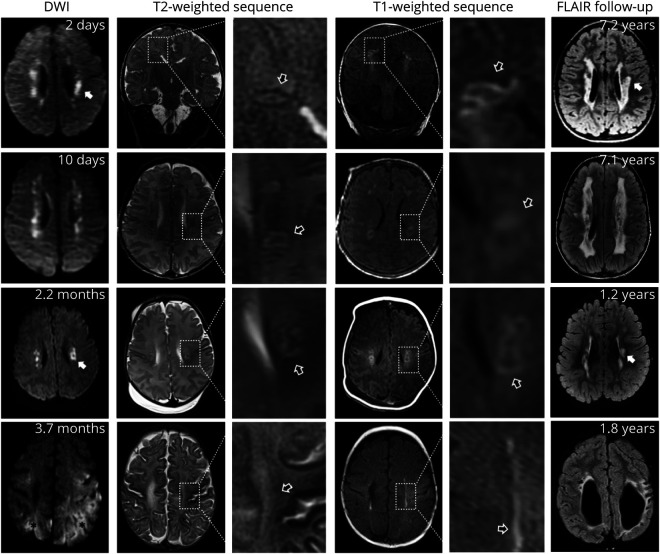
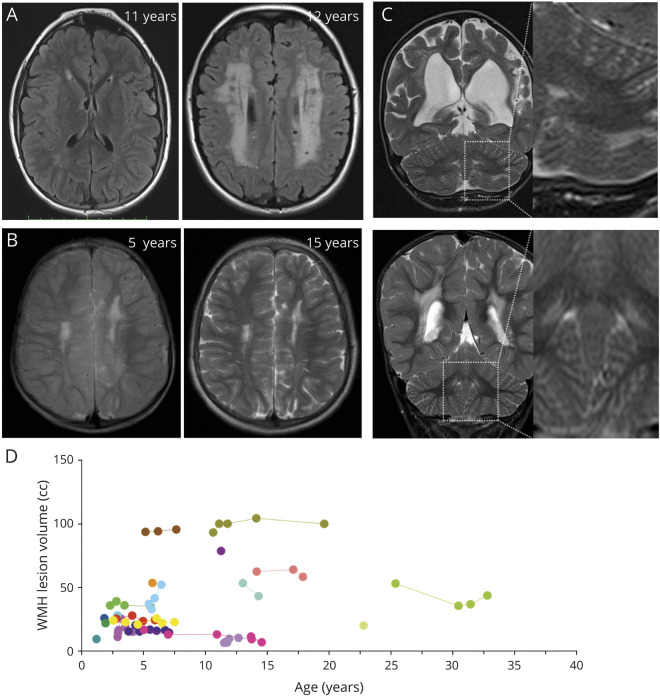
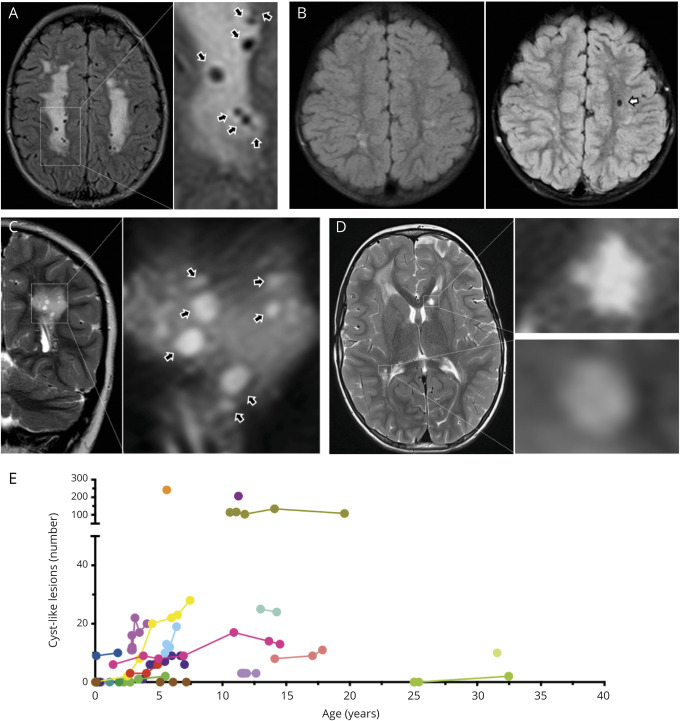
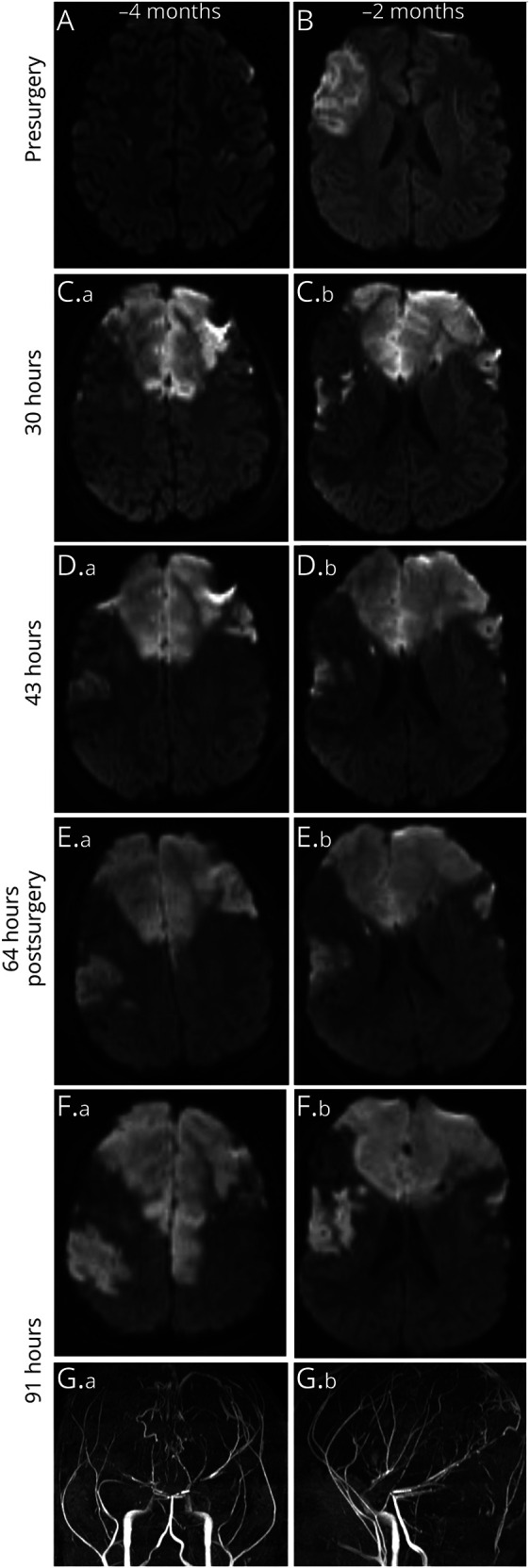
Results: We found characteristic patterns of acute white matter ischemic injury and progressive internal carotid artery stenosis during infancy. Longitudinal analysis of patients older than 1.2 years showed stable white matter hyperintensities but increased number of cystic-like lesions over time. Progressive narrowing of the terminal internal carotid artery occurred in 80% of patients and correlated with the number of critical stenoses in cerebral arteries and arterial ischemic infarctions. Arterial ischemic strokes occurred in same territories affected by critical stenosis.
Conclusions: We found characteristic, early, and progressive cerebrovascular abnormalities in patients with ACTA2 Arg179 pathogenic variants. Our longitudinal data suggest that while steno-occlusive disease progresses over time and is associated with arterial ischemic infarctions and cystic-like white matter lesions, white matter hyperintensities can remain stable over long periods. The evaluated metrics will enable diagnosis in early infancy and be used to monitor disease progression, guide timing of stroke preventive interventions, and assess response to current and future therapies.
© 2020 American Academy of Neurology.
Figures

References
-
- Milewicz DM, Kwartler CS, Papke CL, Regalado ES, Cao J, Reid AJ. Genetic variants promoting smooth muscle cell proliferation can result in diffuse and diverse vascular diseases: evidence for a hyperplastic vasculomyopathy. Genet Med 2010;12:196–203. - PubMed
-
- Meuwissen MEC, Lequin MH, Bindels-de Heus K, et al. . ACTA2 mutation with childhood cardiovascular, autonomic and brain anomalies and severe outcome. Am J Med Genet A 2013;161A:1376–1380. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous