

The Impact of Liver Transplantation on Hepatocellular Carcinoma Mortality in the United States
- PMID: 33199438
- PMCID: PMC8052263
- DOI: 10.1158/1055-9965.EPI-20-1188
The Impact of Liver Transplantation on Hepatocellular Carcinoma Mortality in the United States
Abstract
Background: Hepatocellular carcinoma (HCC) carries a poor prognosis. Liver transplantation (LT) is potentially curative for localized HCC. We evaluated the impact of LT on U.S. general population HCC-specific mortality rates.
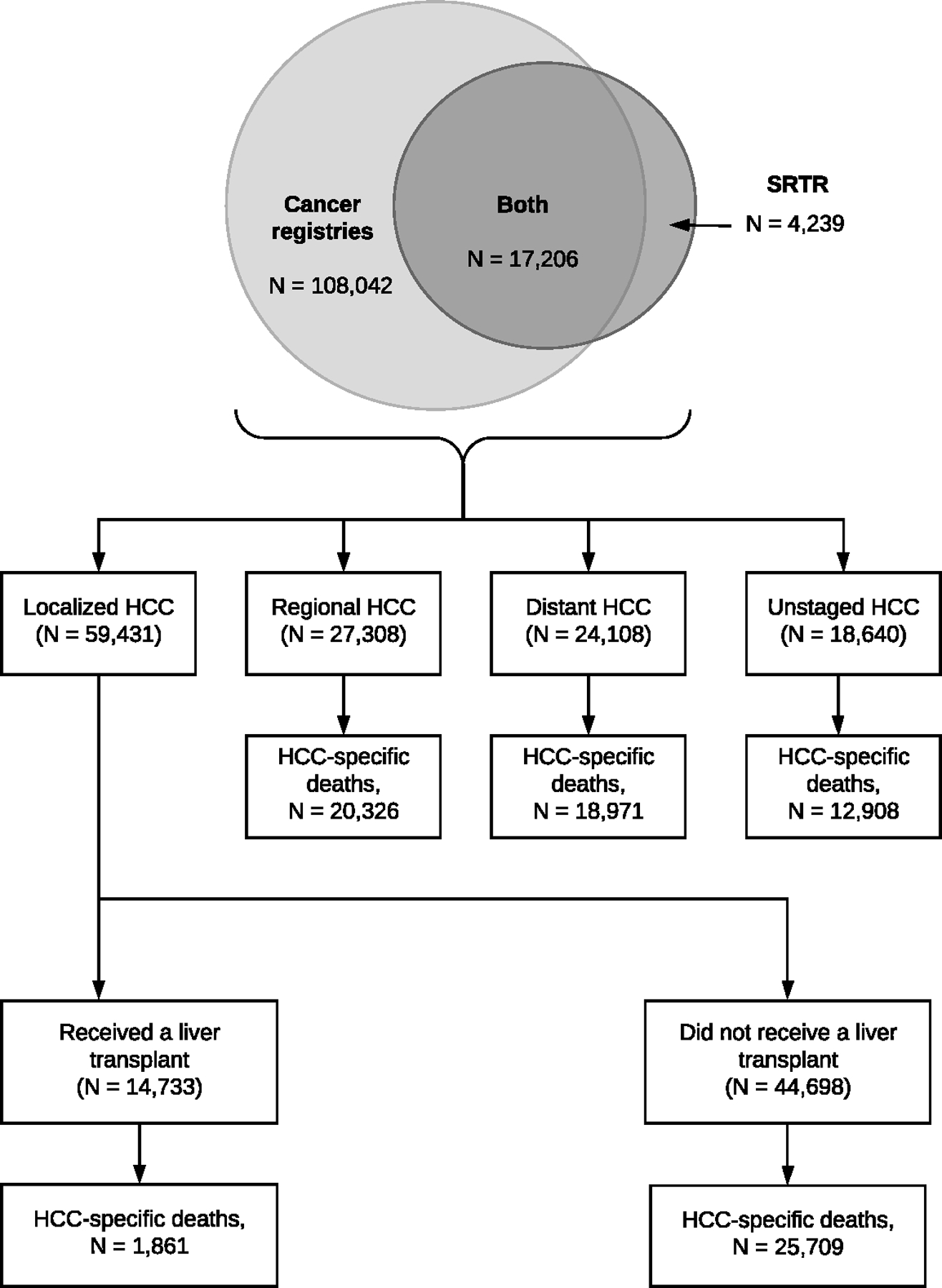
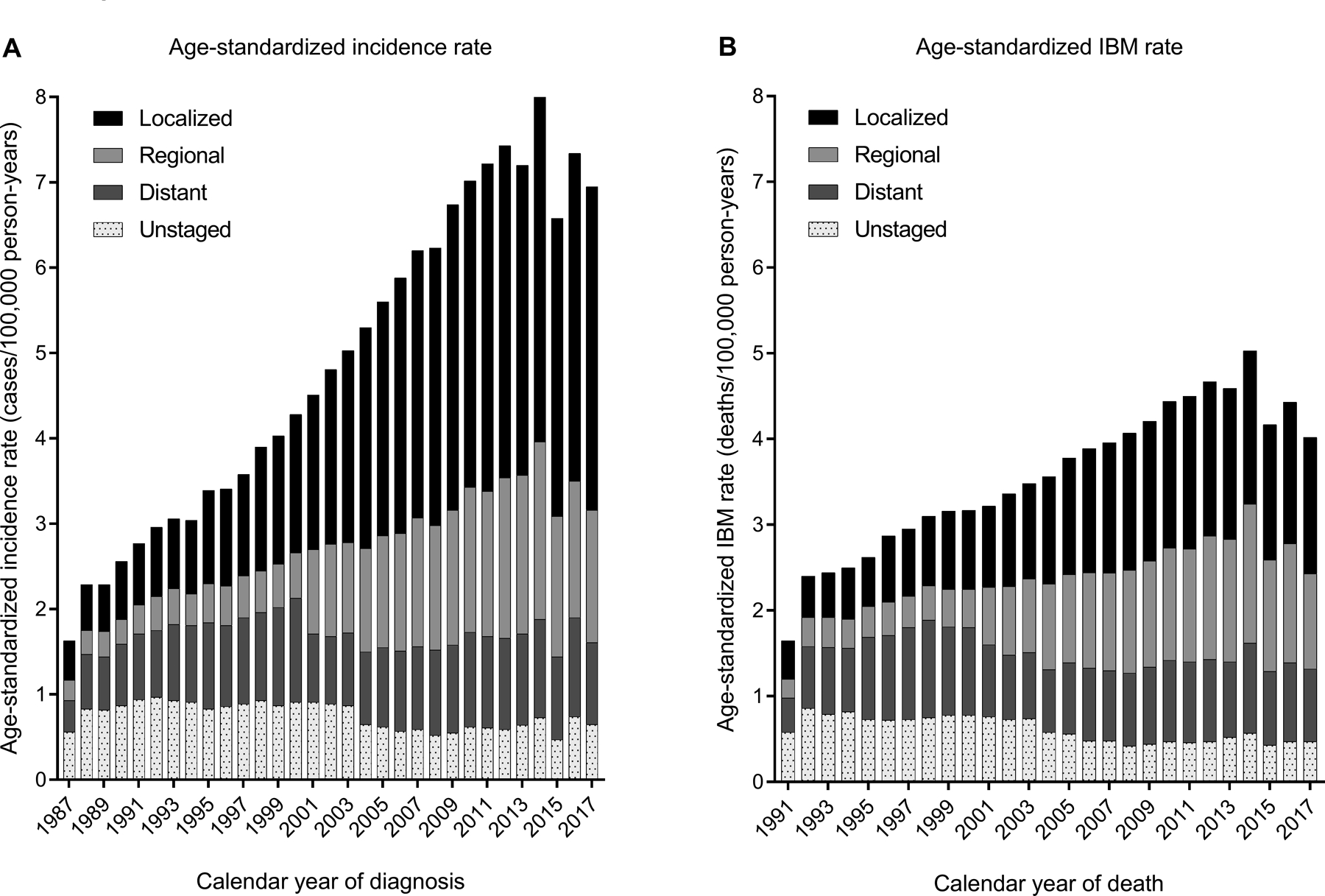
Methods: The Transplant Cancer Match Study links the U.S. transplant registry with 17 cancer registries. We calculated age-standardized incidence (1987-2017) and incidence-based mortality (IBM) rates (1991-2017) for adult HCCs. We partitioned population-level IBM rates by cancer stage and calculated counterfactual IBM rates assuming transplanted cases had not received a transplant.
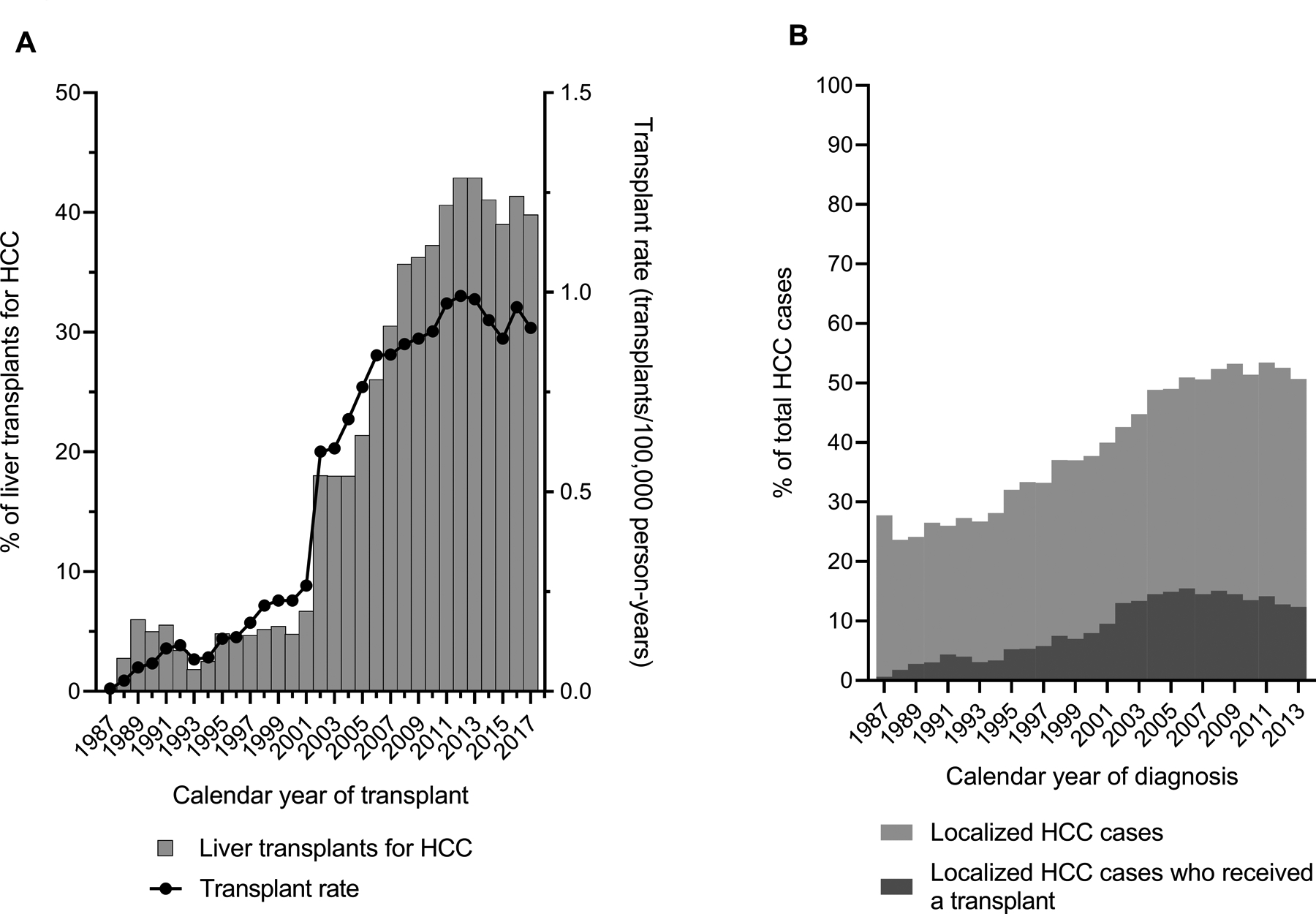
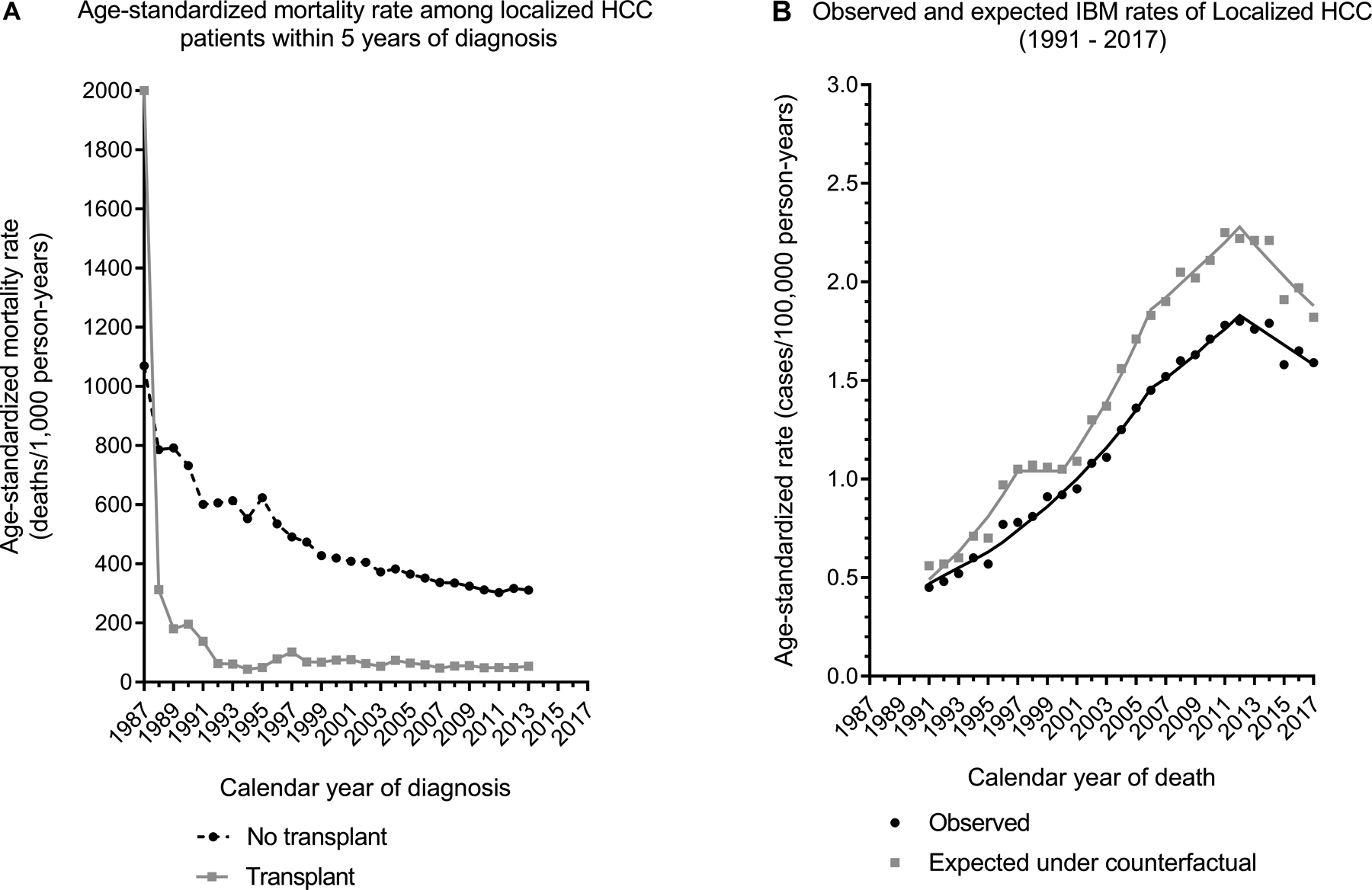
Results: Among 129,487 HCC cases, 45.9% had localized cancer. HCC incidence increased on average 4.0% annually [95% confidence interval (CI) = 3.6-4.5]. IBM also increased for HCC overall (2.9% annually; 95% CI = 1.7-4.2) and specifically for localized stage HCC (4.8% annually; 95% CI = 4.0-5.5). The proportion of HCC-related transplants jumped sharply from 6.7% (2001) to 18.0% (2002), and further increased to 40.0% (2017). HCC-specific mortality declined among both nontransplanted and transplanted cases over time. In the absence of transplants, IBM for localized HCC would have increased at 5.3% instead of 4.8% annually.
Conclusions: LT has provided survival benefit to patients with localized HCC. However, diagnosis of many cases at advanced stages, limited availability of donor livers, and improved mortality for patients without transplants have limited the impact of transplantation on general population HCC-specific mortality rates.
Impact: Although LT rates continue to rise, better screening and treatment modalities are needed to halt the rising HCC mortality rates in the United States.See related commentary by Zhang and Thrift, p. 435.
©2020 American Association for Cancer Research.
Conflict of interest statement
Figures
Comment in
-
Modest Impact of Liver Transplantation on Hepatocellular Carcinoma Mortality in the United States, Findings from The Transplant Cancer Match (TCM) Study.Cancer Epidemiol Biomarkers Prev. 2021 Mar;30(3):435-437. doi: 10.1158/1055-9965.EPI-20-1569. Cancer Epidemiol Biomarkers Prev. 2021. PMID: 33857017
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68(6):394–424 - PubMed
-
- Marrero JA, Kulik LM, Sirlin CB, Zhu AX, Finn RS, Abecassis MM, et al. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018;68(2):723–50 - PubMed
-
- Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med 1996;334(11):693–9 - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN261201800005C/CA/NCI NIH HHS/United States
- U58 DP003875/DP/NCCDPHP CDC HHS/United States
- HHSN261201000036C/CA/NCI NIH HHS/United States
- U58 DP000807/DP/NCCDPHP CDC HHS/United States
- U58 DP000848/DP/NCCDPHP CDC HHS/United States
- Z99 CA999999/ImNIH/Intramural NIH HHS/United States
- HHSN261201800002C/CA/NCI NIH HHS/United States
- U58 DP000824/DP/NCCDPHP CDC HHS/United States
- HHSN261201800002B/CA/NCI NIH HHS/United States
- U58 DP003883/DP/NCCDPHP CDC HHS/United States
- N01 PC035143/CA/NCI NIH HHS/United States
- HHSN261201300021C/CA/NCI NIH HHS/United States
- HHSN261201000035I/CA/NCI NIH HHS/United States
- HHSN261201000035C/PC/NCI NIH HHS/United States
- HHSN261201000034C/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
