

Randomized Phase II and Biomarker Study of Pembrolizumab plus Bevacizumab versus Pembrolizumab Alone for Patients with Recurrent Glioblastoma
- PMID: 33199490
- PMCID: PMC8284901
- DOI: 10.1158/1078-0432.CCR-20-2500
Randomized Phase II and Biomarker Study of Pembrolizumab plus Bevacizumab versus Pembrolizumab Alone for Patients with Recurrent Glioblastoma
Abstract
Purpose: VEGF is upregulated in glioblastoma and may contribute to immunosuppression. We performed a phase II study of pembrolizumab alone or with bevacizumab in recurrent glioblastoma.
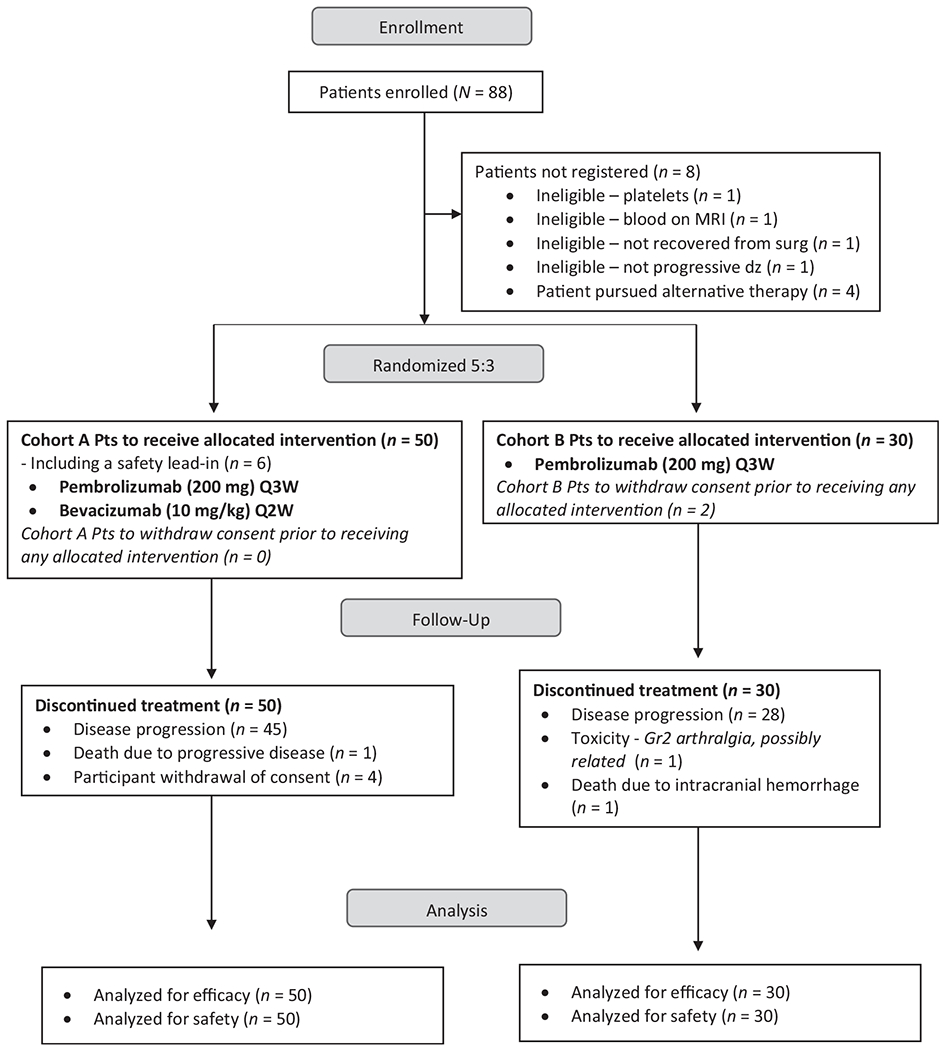
Patients and methods: Eighty bevacizumab-naïve patients with recurrent glioblastoma were randomized to pembrolizumab with bevacizumab (cohort A, n = 50) or pembrolizumab monotherapy (cohort B, n = 30). The primary endpoint was 6-month progression-free survival (PFS-6). Assessed biomarkers included evaluation of tumor programmed death-ligand 1 expression, tumor-infiltrating lymphocyte density, immune activation gene expression signature, and plasma cytokines. The neurologic assessment in neuro-oncology (NANO) scale was used to prospectively assess neurologic function.
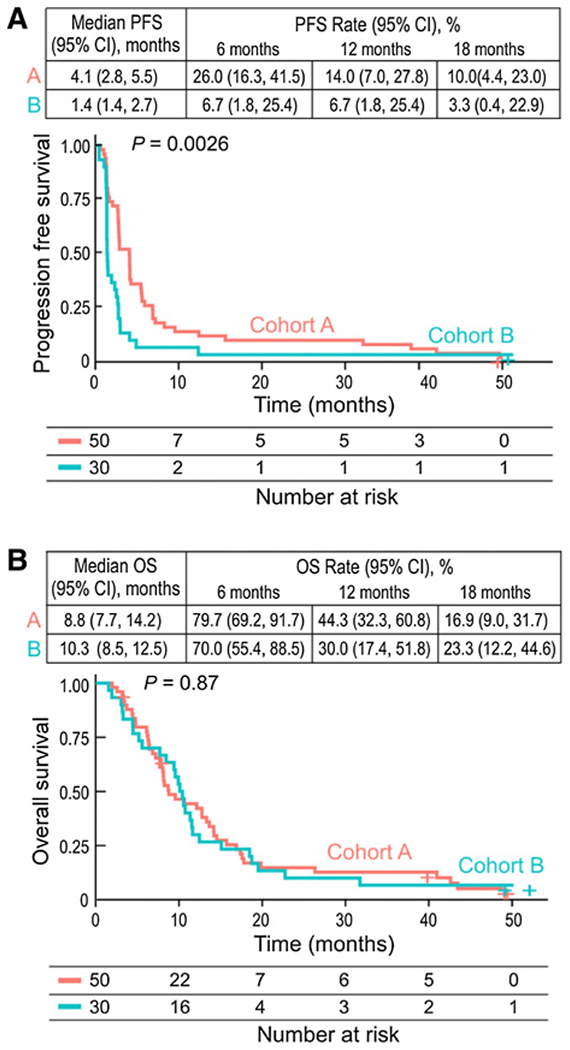
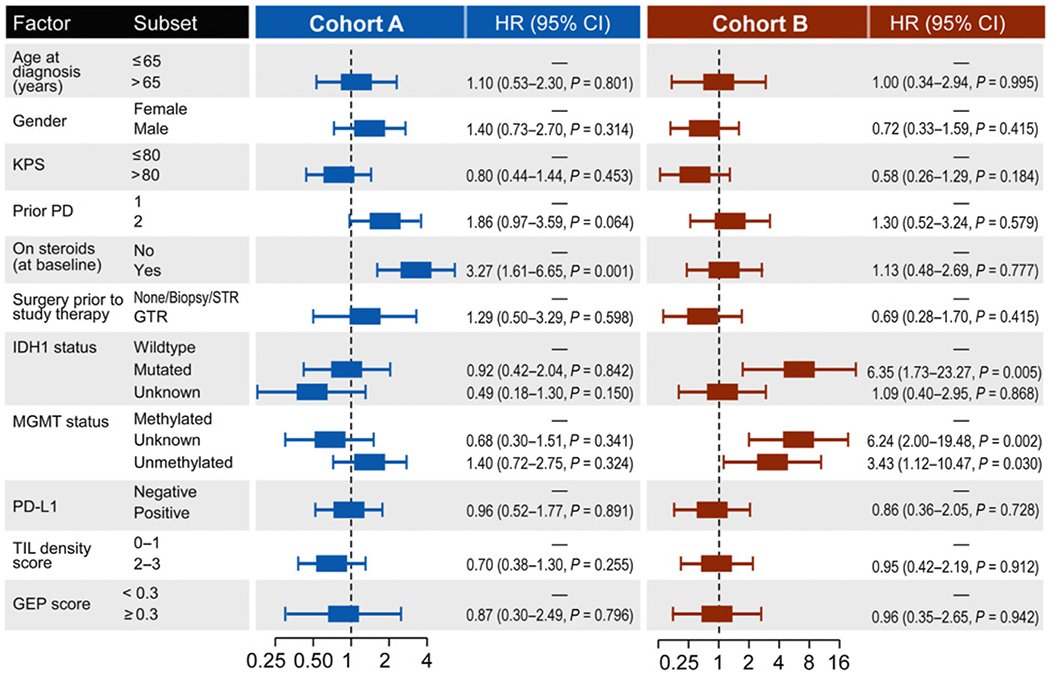
Results: Pembrolizumab alone or with bevacizumab was well tolerated but of limited benefit. For cohort A, PFS-6 was 26.0% [95% confidence interval (CI), 16.3-41.5], median overall survival (OS) was 8.8 months (95% CI, 7.7-14.2), objective response rate (ORR) was 20%, and median duration of response was 48 weeks. For cohort B, PFS-6 was 6.7% (95% CI, 1.7-25.4), median OS was 10.3 months (95% CI, 8.5-12.5), and ORR was 0%. Tumor immune markers were not associated with OS, but worsened OS correlated with baseline dexamethasone use and increased posttherapy plasma VEGF (cohort A) and mutant IDH1, unmethylated MGMT, and increased baseline PlGF and sVEGFR1 levels (cohort B). The NANO scale contributed to overall outcome assessment.
Conclusions: Pembrolizumab was ineffective as monotherapy and with bevacizumab for recurrent glioblastoma. The infrequent radiographic responses to combinatorial therapy were durable. Tumor immune biomarkers did not predict outcome. Baseline dexamethasone use and tumor MGMT warrant further study as potential biomarkers in glioblastoma immunotherapy trials.
©2020 American Association for Cancer Research.
Figures
References
-
- Weller M, Butowski N, Tran DD, Recht LD, Lim M, Hirte H, et al. Rindopepimut with temozolomide for patients with newly diagnosed, EGFRvIII-expressing glioblastoma (ACT IV): a randomised, double-blind, international phase 3 trial. Lancet Oncol 2017;18:1373–85. - PubMed
-
- Mangani D, Weller M, Roth P. The network of immunosuppressive pathways in glioblastoma. Biochem Pharmacol 2017;130:1–9. - PubMed
-
- Wick W, Gorlia T, Bendszus M, Taphoorn M, Sahm F, Harting I, et al. Lomustine and bevacizumab in progressive glioblastoma. N Engl J Med 2017;377:1954–63. - PubMed
-
- Chinot OL, Wick W, Mason W, Henriksson R, Saran F, Nishikawa R, et al. Bevacizumab plus radiotherapy-temozolomide for newly diagnosed glioblastoma. N Engl J Med 2014;370:709–22. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
