

Ethnicity and clinical outcomes in COVID-19: A systematic review and meta-analysis
- PMID: 33200120
- PMCID: PMC7658622
- DOI: 10.1016/j.eclinm.2020.100630
Ethnicity and clinical outcomes in COVID-19: A systematic review and meta-analysis
Abstract
Background: Patients from ethnic minority groups are disproportionately affected by Coronavirus disease (COVID-19). We performed a systematic review and meta-analysis to explore the relationship between ethnicity and clinical outcomes in COVID-19.
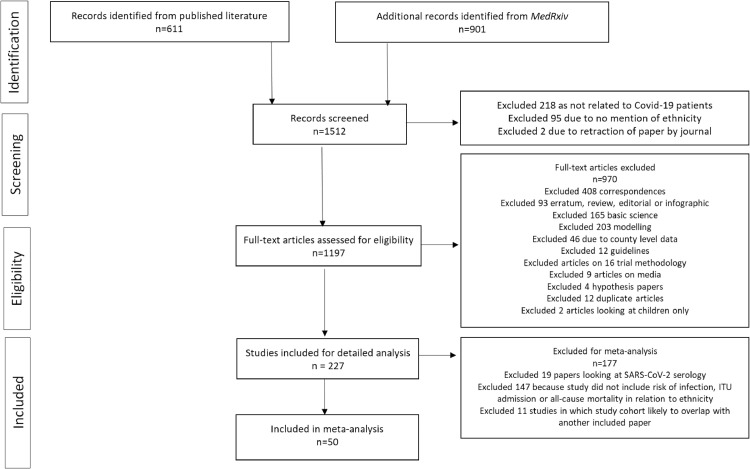
Methods: Databases (MEDLINE, EMBASE, PROSPERO, Cochrane library and MedRxiv) were searched up to 31st August 2020, for studies reporting COVID-19 data disaggregated by ethnicity. Outcomes were: risk of infection; intensive therapy unit (ITU) admission and death. PROSPERO ID: 180654.
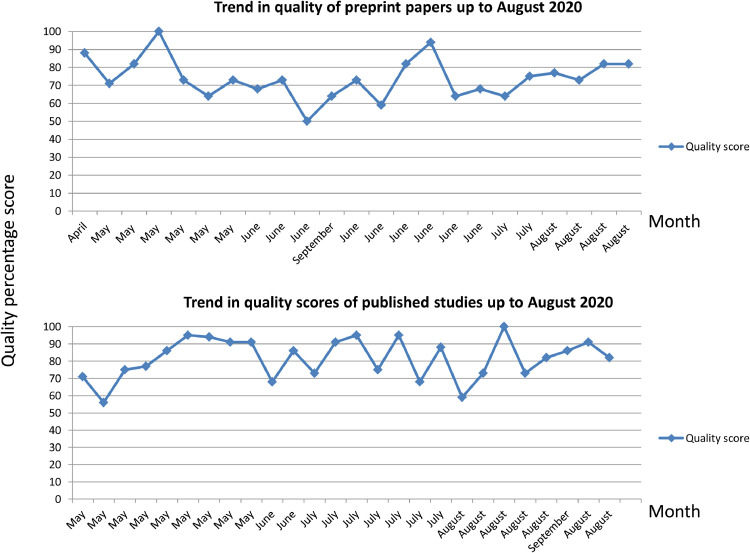
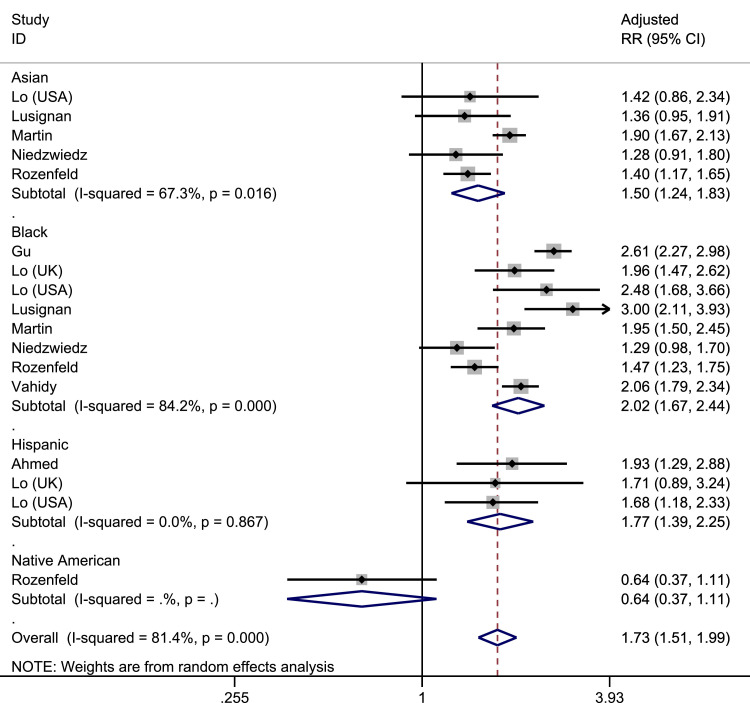
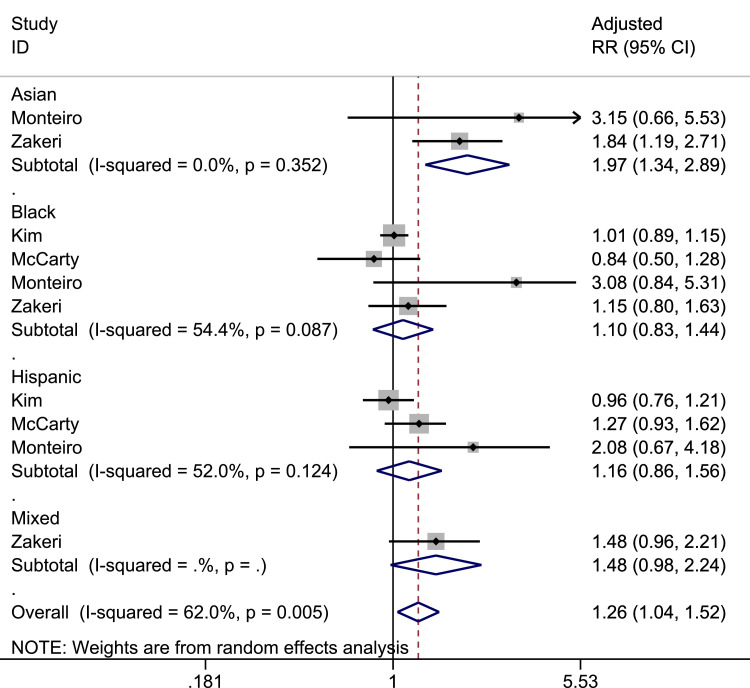
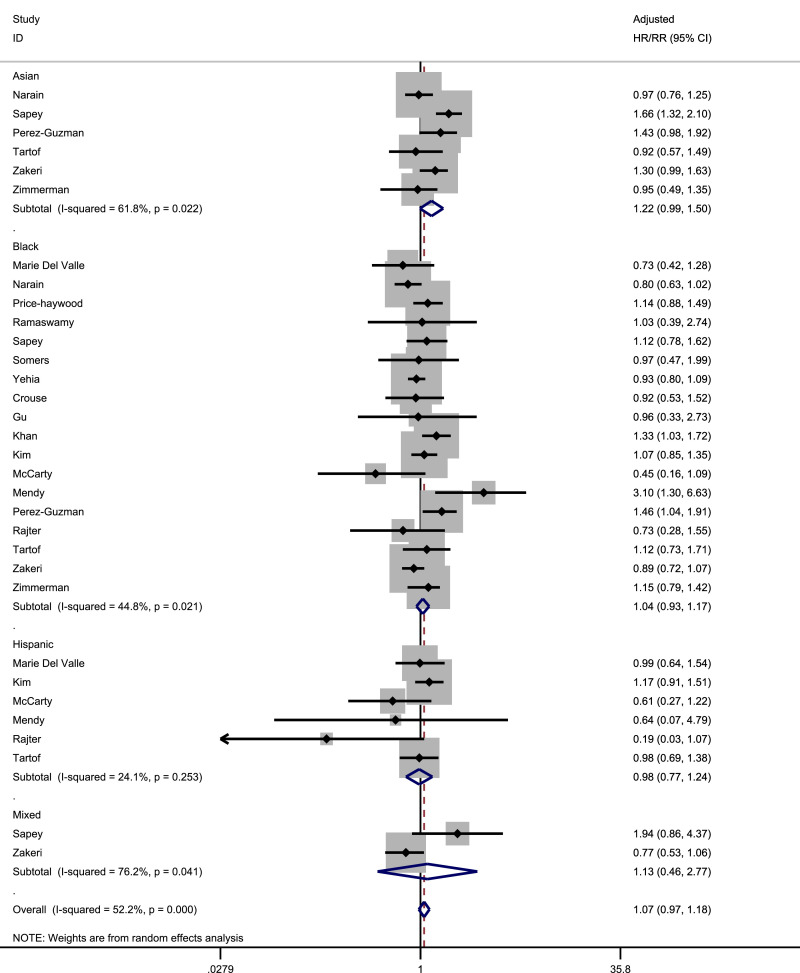
Findings: 18,728,893 patients from 50 studies were included; 26 were peer-reviewed; 42 were from the United States of America and 8 from the United Kingdom. Individuals from Black and Asian ethnicities had a higher risk of COVID-19 infection compared to White individuals. This was consistent in both the main analysis (pooled adjusted RR for Black: 2.02, 95% CI 1.67-2.44; pooled adjusted RR for Asian: 1.50, 95% CI 1.24-1.83) and sensitivity analyses examining peer-reviewed studies only (pooled adjusted RR for Black: 1.85, 95%CI: 1.46-2.35; pooled adjusted RR for Asian: 1.51, 95% CI 1.22-1.88). Individuals of Asian ethnicity may also be at higher risk of ITU admission (pooled adjusted RR 1.97 95% CI 1.34-2.89) (but no studies had yet been peer-reviewed) and death (pooled adjusted RR/HR 1.22 [0.99-1.50]).
Interpretation: Individuals of Black and Asian ethnicity are at increased risk of COVID-19 infection compared to White individuals; Asians may be at higher risk of ITU admission and death. These findings are of critical public health importance in informing interventions to reduce morbidity and mortality amongst ethnic minority groups.
Keywords: Asian; COVID-19 Black; Hispanic; ITU admission; SARS-CoV-2; death; disporportionate; ethnic; ethnicity; infection; outcome; race; transmission.
© 2020 The Author(s).
Conflict of interest statement
KRA has served as a paid consultant, providing unrelated methodological advice, to; Abbvie, Amaris, Allergan, Astellas, AstraZeneca, Boehringer Ingelheim, Bristol-Meyers Squibb, Creativ-Ceutical, GSK, ICON/Oxford Outcomes, Ipsen, Janssen, Eli Lilly, Merck, NICE, Novartis, NovoNordisk, Pfizer, PRMA, Roche and Takeda, and has received research funding from Association of the British Pharmaceutical Industry (ABPI), European Federation of Pharmaceutical Industries & Associations (EFPIA), Pfizer, Sanofi and Swiss Precision Diagnostics. He is a Partner and Director of Visible Analytics Limited, a healthcare consultancy company. KK has received honoraria from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Janssen, Merck Sharp & Dohme, Novartis, Novo Nordisk, Sanofi, Takeda, Servier and Pfizer, and research support from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Novartis, Novo Nordisk, Sanofi and Pfizer. KK is Director for the University of Leicester Centre for BME Health, Trustee of the South Asian Health Foundation, national NIHR ARC lead for Ethnicity and Diversity, Chair of the SAGE subgroup on Ethnicity and COVD and a member of Independent SAGE. MP reports grants and personal fees from Gilead Sciences and personal fees from QIAGEN, outside the submitted work. All other authors report no conflict of interest.
Figures
Comment in
-
Use of BAME is controversial-occupational risk from COVID-19 and supporting ethnic minority workers.Occup Med (Lond). 2022 Feb 22;72(2):65-66. doi: 10.1093/occmed/kqab067. Occup Med (Lond). 2022. PMID: 34551111 Free PMC article. No abstract available.
References
-
- Johns Hopkins University of Medicie Coronavirus Resource Center. COVID-19 dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). https://coronavirus.jhu.edu/map.html (accessed Sept 4, 2020).
-
- Williams D., Cooper L. COVID-19 and health equity – a new kind of ‘herd immunity’. JAMA. 2020;323:2478–2480. - PubMed
-
- Yancy C.W. COVID-19 and African Americans. JAMA – J Am Med Assoc. 2020;323:1891–1892. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
