

This is a preprint.
Seasonal human coronavirus antibodies are boosted upon SARS-CoV-2 infection but not associated with protection
- PMID: 33200143
- PMCID: PMC7668756
- DOI: 10.1101/2020.11.06.20227215
Seasonal human coronavirus antibodies are boosted upon SARS-CoV-2 infection but not associated with protection
Update in
-
Seasonal human coronavirus antibodies are boosted upon SARS-CoV-2 infection but not associated with protection.Cell. 2021 Apr 1;184(7):1858-1864.e10. doi: 10.1016/j.cell.2021.02.010. Epub 2021 Feb 9. Cell. 2021. PMID: 33631096 Free PMC article.
Abstract
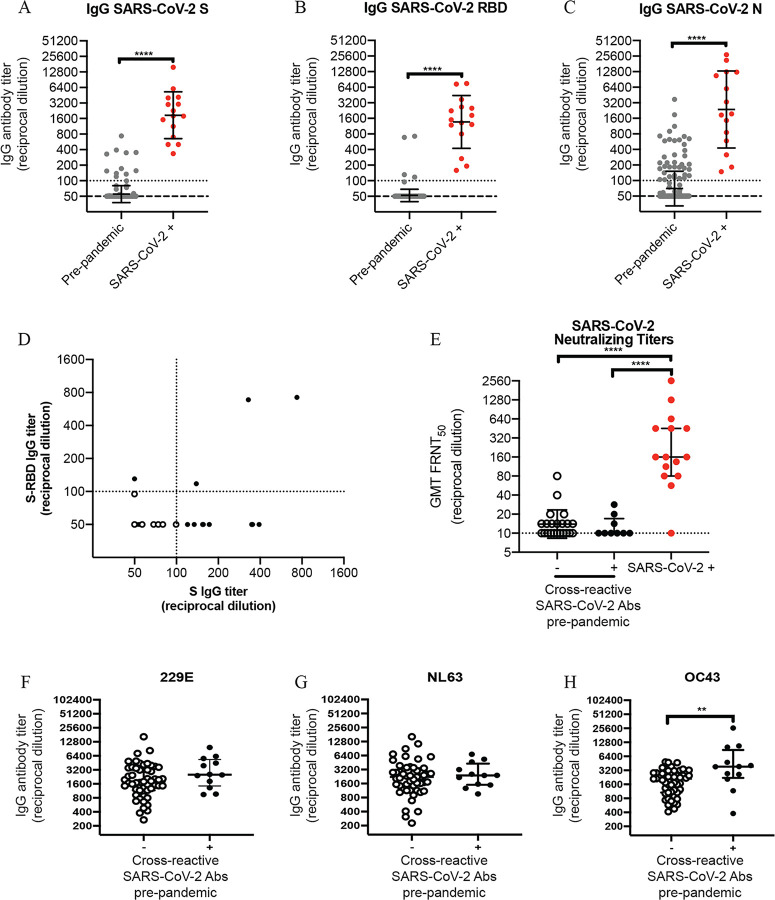
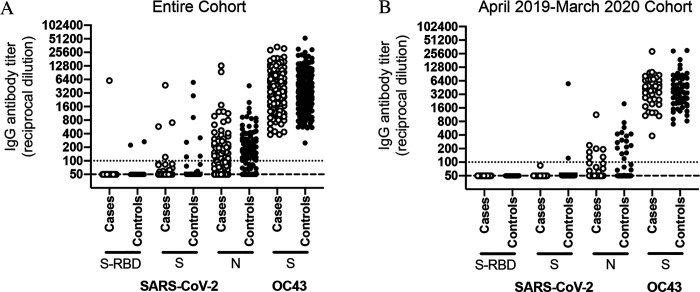
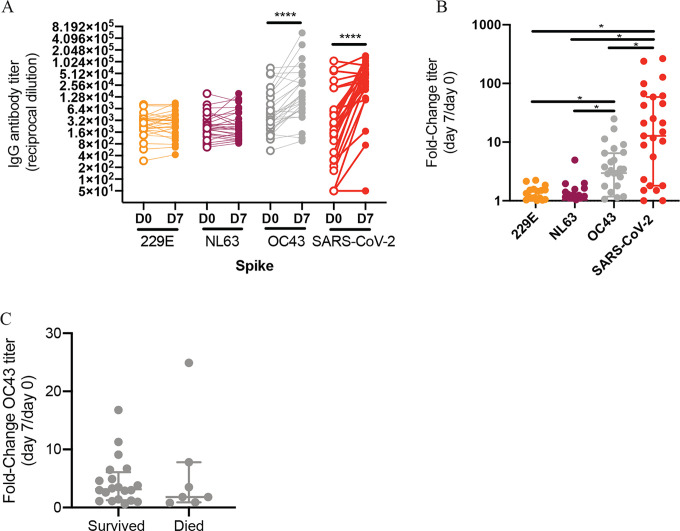
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has rapidly spread within the human population. Although SARS-CoV-2 is a novel coronavirus, most humans had been previously exposed to other antigenically distinct common seasonal human coronaviruses (hCoVs) before the COVID-19 pandemic. Here, we quantified levels of SARS-CoV-2-reactive antibodies and hCoV-reactive antibodies in serum samples collected from 204 humans before the COVID-19 pandemic. We then quantified pre-pandemic antibody levels in serum from a separate cohort of 252 individuals who became PCR-confirmed infected with SARS-CoV-2. Finally, we longitudinally measured hCoV and SARS-CoV-2 antibodies in the serum of hospitalized COVID-19 patients. Our studies indicate that most individuals possessed hCoV-reactive antibodies before the COVID-19 pandemic. We determined that ~23% of these individuals possessed non-neutralizing antibodies that cross-reacted with SARS-CoV-2 spike and nucleocapsid proteins. These antibodies were not associated with protection against SARS-CoV-2 infections or hospitalizations, but paradoxically these hCoV cross-reactive antibodies were boosted upon SARS-CoV-2 infection.
Keywords: COVID-19; SARS-CoV-2; antibody; coronavirus.
Figures
References
-
- Gaunt E. R., Hardie A., Claas E. C., Simmonds P. & Templeton K. E. Epidemiology and clinical presentations of the four human coronaviruses 229E, HKU1, NL63, and OC43 detected over 3 years using a novel multiplex real-time PCR method. J Clin Microbiol 48, 2940–2947, doi:10.1128/JCM.00636-10 (2010). - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous