

Whole-Volume Tumor MRI Radiomics for Prognostic Modeling in Endometrial Cancer
- PMID: 33200420
- PMCID: PMC7894560
- DOI: 10.1002/jmri.27444
Whole-Volume Tumor MRI Radiomics for Prognostic Modeling in Endometrial Cancer
Abstract
Background: In endometrial cancer (EC), preoperative pelvic MRI is recommended for local staging, while final tumor stage and grade are established by surgery and pathology. MRI-based radiomic tumor profiling may aid in preoperative risk-stratification and support clinical treatment decisions in EC.
Purpose: To develop MRI-based whole-volume tumor radiomic signatures for prediction of aggressive EC disease.
Study type: Retrospective.
Population: A total of 138 women with histologically confirmed EC, divided into training (nT = 108) and validation cohorts (nV = 30).
Field strength/sequence: Axial oblique T1 -weighted gradient echo volumetric interpolated breath-hold examination (VIBE) at 1.5T (71/138 patients) and DIXON VIBE at 3T (67/138 patients) at 2 minutes postcontrast injection.
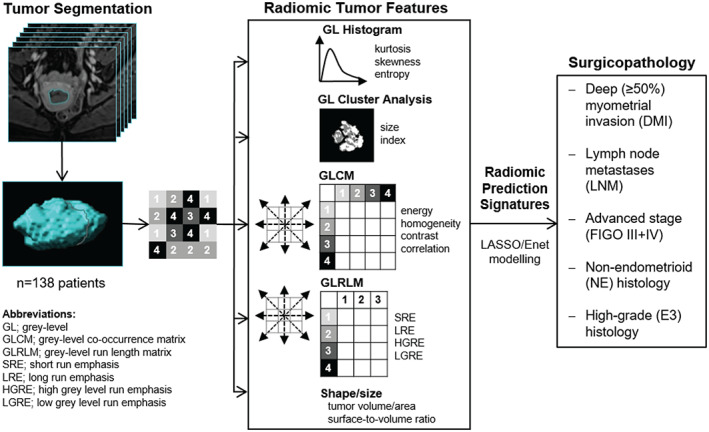
Assessment: Primary tumors were manually segmented by two radiologists with 4 and 8 years' of experience. Radiomic tumor features were computed and used for prediction of surgicopathologically-verified deep (≥50%) myometrial invasion (DMI), lymph node metastases (LNM), advanced stage (FIGO III + IV), nonendometrioid (NE) histology, and high-grade endometrioid tumors (E3). Corresponding analyses were also conducted using radiomics extracted from the axial oblique image slice depicting the largest tumor area.
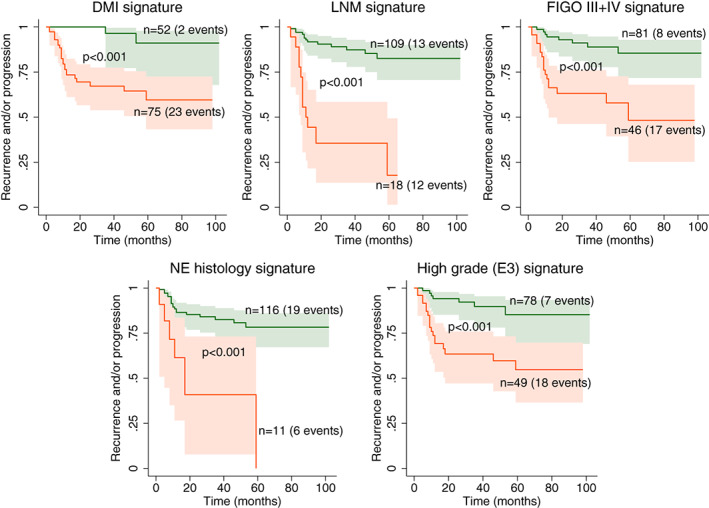
Statistical tests: Logistic least absolute shrinkage and selection operator (LASSO) was applied for radiomic modeling in the training cohort. The diagnostic performances of the radiomic signatures were evaluated by area under the receiver operating characteristic curve in the training (AUCT ) and validation (AUCV ) cohorts. Progression-free survival was assessed using the Kaplan-Meier and Cox proportional hazard model.
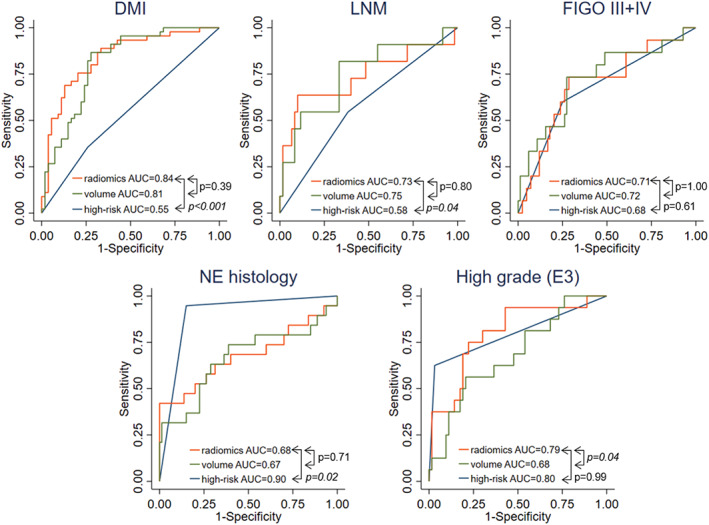
Results: The whole-tumor radiomic signatures yielded AUCT /AUCV of 0.84/0.76 for predicting DMI, 0.73/0.72 for LNM, 0.71/0.68 for FIGO III + IV, 0.68/0.74 for NE histology, and 0.79/0.63 for high-grade (E3) tumor. Single-slice radiomics yielded comparable AUCT but significantly lower AUCV for LNM and FIGO III + IV (both P < 0.05). Tumor volume yielded comparable AUCT to the whole-tumor radiomic signatures for prediction of DMI, LNM, FIGO III + IV, and NE, but significantly lower AUCT for E3 tumors (P < 0.05). All of the whole-tumor radiomic signatures significantly predicted poor progression-free survival with hazard ratios of 4.6-9.8 (P < 0.05 for all).
Data conclusion: MRI-based whole-tumor radiomic signatures yield medium-to-high diagnostic performance for predicting aggressive EC disease. The signatures may aid in preoperative risk assessment and hence guide personalized treatment strategies in EC.
Level of evidence: 4 TECHNICAL EFFICACY STAGE: 2.
Keywords: LASSO regression; MRI; endometrial cancer; prognostic modeling; radiomics.
© 2020 The Authors. Journal of Magnetic Resonance Imaging published by Wiley Periodicals LLC. on behalf of International Society for Magnetic Resonance in Medicine.
Figures
Similar articles
-
MRI-based radiomic signatures for pretreatment prognostication in cervical cancer.Cancer Med. 2023 Oct;12(20):20251-20265. doi: 10.1002/cam4.6526. Epub 2023 Oct 16. Cancer Med. 2023. PMID: 37840437 Free PMC article.
-
MRI delta radiomics during chemoradiotherapy for prognostication in locally advanced cervical cancer.BMC Cancer. 2025 Jan 22;25(1):122. doi: 10.1186/s12885-025-13509-1. BMC Cancer. 2025. PMID: 39844102 Free PMC article.
-
MRI-based radiomics nomogram for the preoperative prediction of deep myometrial invasion of FIGO stage I endometrial carcinoma.Med Phys. 2022 Oct;49(10):6505-6516. doi: 10.1002/mp.15835. Epub 2022 Aug 15. Med Phys. 2022. PMID: 35758644
-
Preoperative risk assessment of invasive endometrial cancer using MRI-based radiomics: a systematic review and meta-analysis.Abdom Radiol (NY). 2025 May 24. doi: 10.1007/s00261-025-05005-8. Online ahead of print. Abdom Radiol (NY). 2025. PMID: 40411548 Review.
-
Preoperative Imaging Evaluation of Endometrial Cancer in FIGO 2023.J Magn Reson Imaging. 2024 Oct;60(4):1225-1242. doi: 10.1002/jmri.29161. Epub 2023 Dec 26. J Magn Reson Imaging. 2024. PMID: 38146775 Review.
Cited by
-
A prediction model based on deep learning and radiomics features of DWI for the assessment of microsatellite instability in endometrial cancer.Cancer Med. 2024 Aug;13(16):e70046. doi: 10.1002/cam4.70046. Cancer Med. 2024. PMID: 39171859 Free PMC article.
-
Impact of MRI radiomic feature normalization for prognostic modelling in uterine endometrial and cervical cancers.Sci Rep. 2024 Jul 22;14(1):16826. doi: 10.1038/s41598-024-66659-w. Sci Rep. 2024. PMID: 39039099 Free PMC article.
-
Evaluation and Monitoring of Endometrial Cancer Based on Magnetic Resonance Imaging Features of Deep Learning.Contrast Media Mol Imaging. 2022 Mar 18;2022:5198592. doi: 10.1155/2022/5198592. eCollection 2022. Contrast Media Mol Imaging. 2022. PMID: 35360265 Free PMC article.
-
Observer- and radiomics model-based computed tomography classification of suppurative versus tuberculous lymphadenitis complicated with nodal necrosis of the neck in children.Pediatr Radiol. 2023 Dec;53(13):2586-2596. doi: 10.1007/s00247-023-05761-z. Epub 2023 Oct 9. Pediatr Radiol. 2023. PMID: 37806973
-
Automatic segmentation of uterine endometrial cancer on multi-sequence MRI using a convolutional neural network.Sci Rep. 2021 Jul 14;11(1):14440. doi: 10.1038/s41598-021-93792-7. Sci Rep. 2021. PMID: 34262088 Free PMC article.
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394‐424. - PubMed
-
- Cancer registry of Norway: Cancer in Norway 2018 — Cancer incidence, mortality, survival and prevalence in Norway. Oslo, Norway: Cancer Registry of Norway; 2019. https://www.kreftregisteret.no/globalassets/cancer-in-norway/2018/cin201....
-
- Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol Obstet 2009;105:103‐104. - PubMed
-
- FIGO staging for carcinoma of the vulva, cervix, and corpus uteri. Int J Gynecol Obstet 2014;125:97‐98. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
