

COVID-19 fatality prediction in people with diabetes and prediabetes using a simple score upon hospital admission
- PMID: 33200501
- PMCID: PMC7753560
- DOI: 10.1111/dom.14256
COVID-19 fatality prediction in people with diabetes and prediabetes using a simple score upon hospital admission
Abstract
Aim: To assess predictors of in-hospital mortality in people with prediabetes and diabetes hospitalized for COVID-19 infection and to develop a risk score for identifying those at the greatest risk of a fatal outcome.
Materials and methods: A combined prospective and retrospective, multicentre, cohort study was conducted at 10 sites in Austria in 247 people with diabetes or newly diagnosed prediabetes who were hospitalized with COVID-19. The primary outcome was in-hospital mortality and the predictor variables upon admission included clinical data, co-morbidities of diabetes or laboratory data. Logistic regression analyses were performed to identify significant predictors and to develop a risk score for in-hospital mortality.
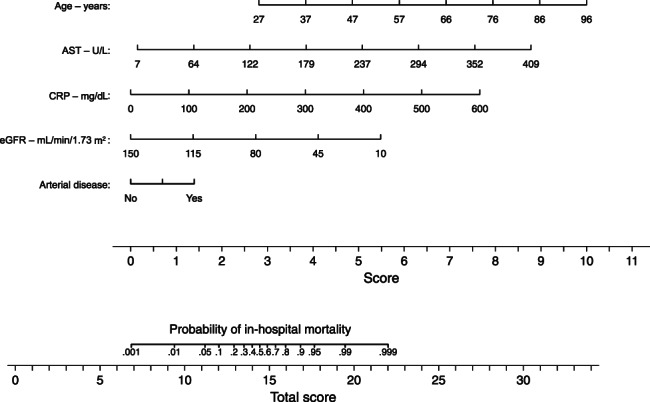
Results: The mean age of people hospitalized (n = 238) for COVID-19 was 71.1 ± 12.9 years, 63.6% were males, 75.6% had type 2 diabetes, 4.6% had type 1 diabetes and 19.8% had prediabetes. The mean duration of hospital stay was 18 ± 16 days, 23.9% required ventilation therapy and 24.4% died in the hospital. The mortality rate in people with diabetes was numerically higher (26.7%) compared with those with prediabetes (14.9%) but without statistical significance (P = .128). A score including age, arterial occlusive disease, C-reactive protein, estimated glomerular filtration rate and aspartate aminotransferase levels at admission predicted in-hospital mortality with a C-statistic of 0.889 (95% CI: 0.837-0.941) and calibration of 1.000 (P = .909).
Conclusions: The in-hospital mortality for COVID-19 was high in people with diabetes but not significantly different to the risk in people with prediabetes. A risk score using five routinely available patient variables showed excellent predictive performance for assessing in-hospital mortality.
Keywords: coronavirus infection, diabetes, prediabetic state.
© 2020 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
H. Sourij received unrestricted research grants from AstraZeneca, Boehringer Ingelheim, Eli Lilly, MSD, NovoNordisk and Sanofi; and received speaker's honoraria from Amgen, AstraZeneca, BMS, Boehringer Ingelheim, Eli Lilly, MSD, NovoNordisk and Sanofi. SK received unrestricted research grants from Boehringer Ingelheim and MSD (CD Laboratory for Metabolic Crosstalk). SK received speaker's honoraria from AstraZeneca, Boehringer Ingelheim, Eli Lilly, MSD, NovoNordisk and Sanofi. CC received speaker's honoraria from AstraZeneca, Boehringer Ingelheim, Eli Lilly, MSD, NovoNordisk and Sanofi. H. Stingl received an unresctricted research grant from Boehringer Ingelheim; and received speaker's honoraria from Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, NovoNordisk, Novartis, and Sanofi Aventis and Servier. CR received speaker's honoraria and congress support from AstraZeneca, NovoNordisk and Sanofi. All the other authors declare no conflicts of interest with regard to this manuscript.
Figures
Similar articles
-
Biomarkers Predictive for In-Hospital Mortality in Patients with Diabetes Mellitus and Prediabetes Hospitalized for COVID-19 in Austria: An Analysis of COVID-19 in Diabetes Registry.Viruses. 2022 Jun 13;14(6):1285. doi: 10.3390/v14061285. Viruses. 2022. PMID: 35746755 Free PMC article.
-
Clinical Characteristics and Outcomes of Patients With Diabetes Admitted for COVID-19 Treatment in Dubai: Single-Centre Cross-Sectional Study.JMIR Public Health Surveill. 2020 Dec 7;6(4):e22471. doi: 10.2196/22471. JMIR Public Health Surveill. 2020. PMID: 33284130 Free PMC article.
-
Clinical characteristics and outcomes of COVID-19 patients with prediabetes.Diabetes Metab Syndr. 2021 Jul-Aug;15(4):102192. doi: 10.1016/j.dsx.2021.102192. Epub 2021 Jun 29. Diabetes Metab Syndr. 2021. PMID: 34224947 Free PMC article.
-
Patients with prediabetes are at greater risk of developing diabetes 5 months postacute SARS-CoV-2 infection: a retrospective cohort study.BMJ Open Diabetes Res Care. 2023 Jun;11(3):e003257. doi: 10.1136/bmjdrc-2022-003257. BMJ Open Diabetes Res Care. 2023. PMID: 37295808 Free PMC article.
-
A UK nationwide study of people with type 1 diabetes admitted to hospital with COVID-19 infection.Diabetologia. 2021 Aug;64(8):1717-1724. doi: 10.1007/s00125-021-05463-x. Epub 2021 May 8. Diabetologia. 2021. PMID: 33966090 Free PMC article.
Cited by
-
Pre-admission glucagon-like peptide-1 receptor agonist (GLP-1RA) and mortality from coronavirus disease 2019 (Covid-19): A systematic review, meta-analysis, and meta-regression.Diabetes Res Clin Pract. 2021 Sep;179:109031. doi: 10.1016/j.diabres.2021.109031. Epub 2021 Aug 28. Diabetes Res Clin Pract. 2021. PMID: 34461139 Free PMC article.
-
The management of type 2 diabetes before, during and after Covid-19 infection: what is the evidence?Cardiovasc Diabetol. 2021 Oct 1;20(1):198. doi: 10.1186/s12933-021-01389-1. Cardiovasc Diabetol. 2021. PMID: 34598700 Free PMC article.
-
Only Subclinical Alterations in the Haemostatic System of People with Diabetes after COVID-19 Vaccination.Viruses. 2022 Dec 20;15(1):10. doi: 10.3390/v15010010. Viruses. 2022. PMID: 36680051 Free PMC article.
-
Noninsulin-based antihyperglycemic medications in patients with diabetes and COVID-19: A systematic review and meta-analysis.J Diabetes. 2023 Feb;15(2):86-96. doi: 10.1111/1753-0407.13359. Epub 2023 Jan 23. J Diabetes. 2023. PMID: 36690377 Free PMC article.
-
Preinfection glycaemic control and disease severity among patients with type 2 diabetes and COVID-19: A retrospective, cohort study.Diabetes Obes Metab. 2021 Aug;23(8):1995-2000. doi: 10.1111/dom.14393. Epub 2021 Apr 16. Diabetes Obes Metab. 2021. PMID: 33822446 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
