

Comparative Safety of Sleeve Gastrectomy and Gastric Bypass: An Instrumental Variables Approach
- PMID: 33201113
- PMCID: PMC11495229
- DOI: 10.1097/SLA.0000000000004297
Comparative Safety of Sleeve Gastrectomy and Gastric Bypass: An Instrumental Variables Approach
Abstract
Objective: To compare the safety of sleeve gastrectomy and gastric bypass in a large cohort of commercially insured bariatric surgery patients from the IBM MarketScan claims database, while accounting for measurable and unmeasurable sources of selection bias in who is chosen for each operation.
Summary of background data: Sleeve gastrectomy has rapidly become the most common bariatric operation performed in the United States, but its longer-term safety is poorly described, and the risk of worsening gastroesophageal reflux requiring revision may be higher than previously thought. Prior studies comparing sleeve gastrectomy to gastric bypass are limited by low sample size (in randomized trials) and selection bias (in observational studies).
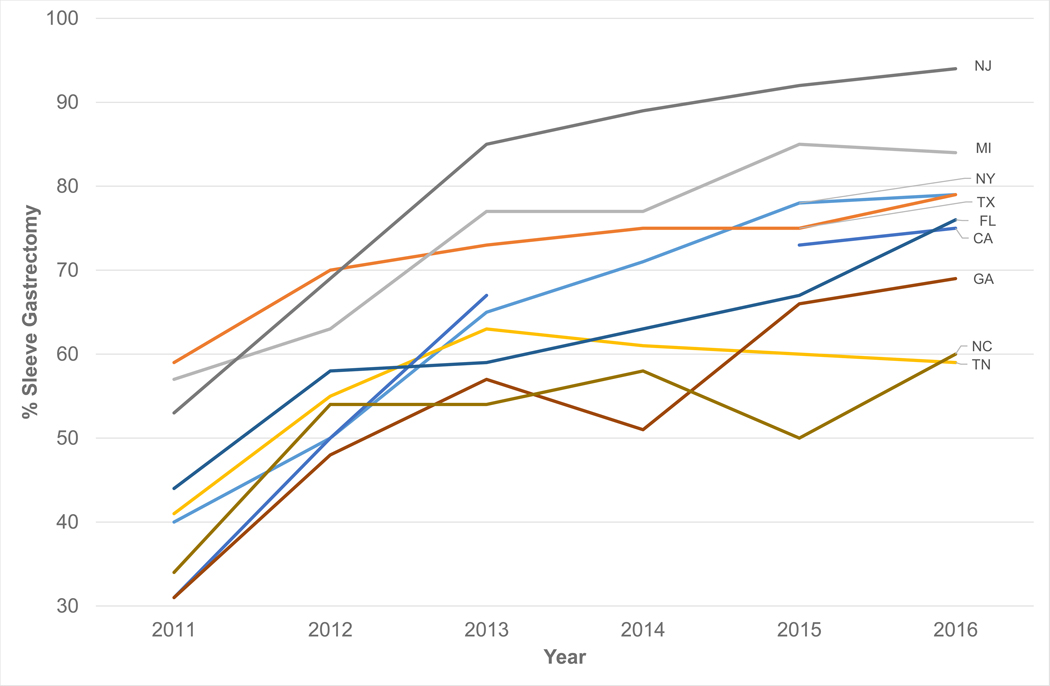
Methods: Instrumental variables analysis of commercially insured patients in the IBM MarketScan claims database from 2011 to 2018. We studied patients undergoing bariatric surgery from 2012 to 2016. We identified re-interventions and complications at 30 days and 2 years from surgery using Comprehensive Procedural Terminology and International Classification of Disease (ICD)-9/10 codes. To overcome unmeasured confounding, we use the prior year's sleeve gastrectomy utilization within each state as an instrumental variable-exploiting variation in the timing of payers' decisions to cover sleeve gastrectomy as a natural experiment.
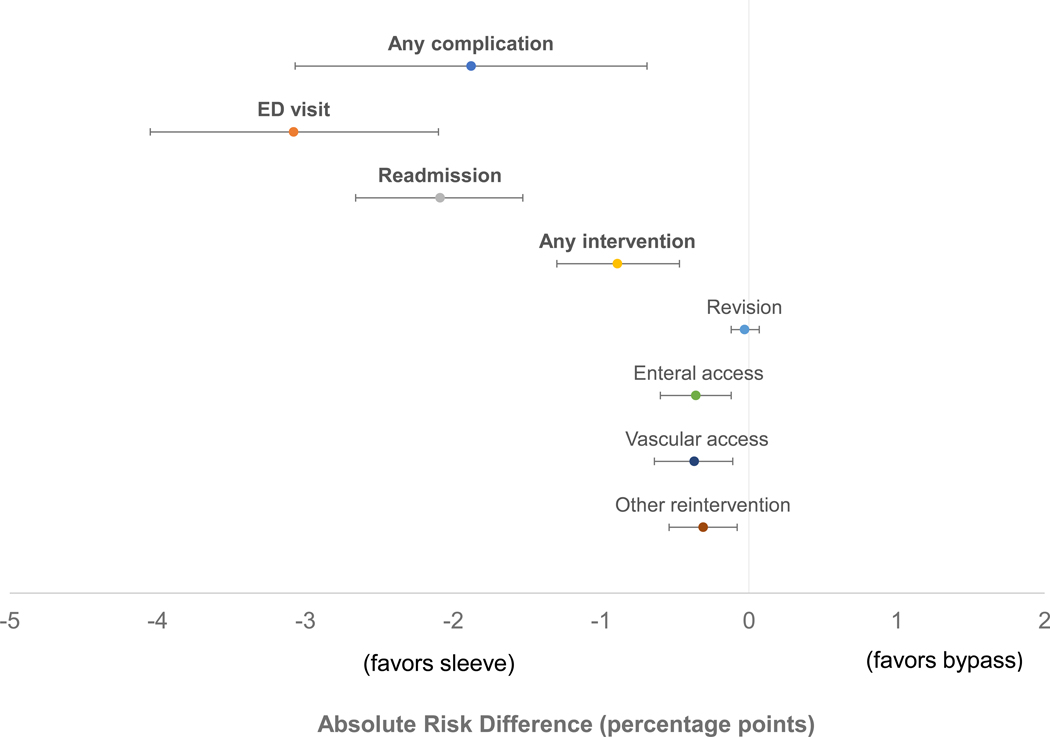
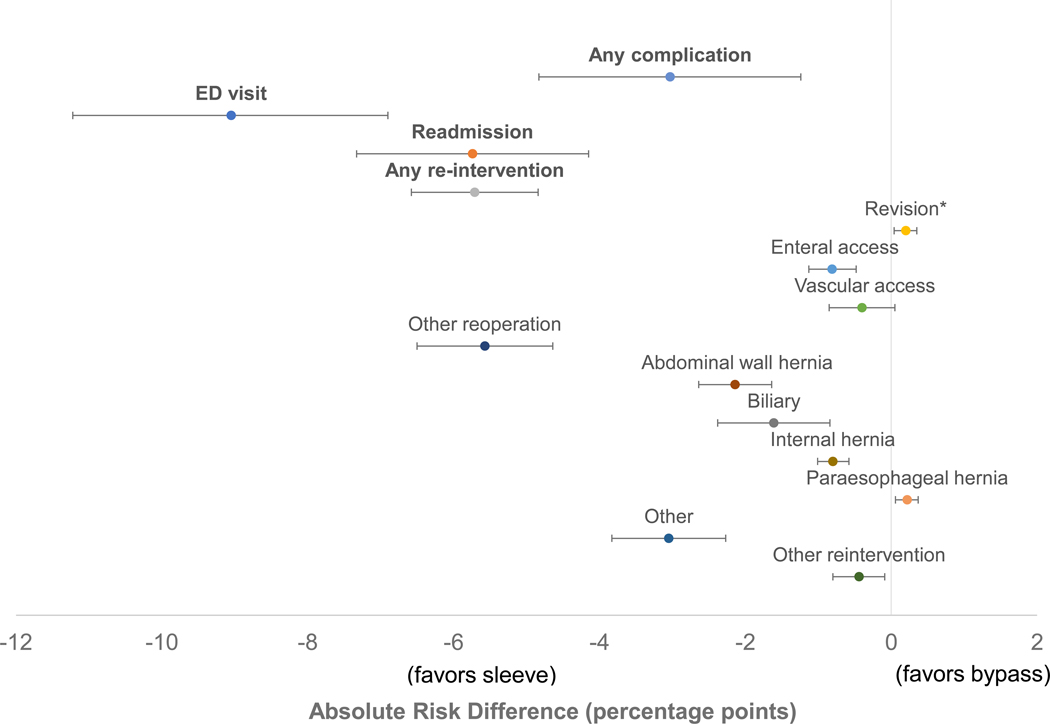
Results: Among 38,153 patients who underwent bariatric surgery between 2012 and 2016, the share of sleeve gastrectomy rose from 52.6% (2012) to 75% (2016). At 2 years from surgery, patients undergoing sleeve gastrectomy had fewer re-interventions (sleeve 9.9%, bypass 15.6%, P < 0.001) and complications (sleeve 6.6%, bypass 9.6%, P = 0.001), and lower overall healthcare spending ($47,891 vs $55,213, P = 0.003), than patients undergoing gastric bypass. However, at the 2-year mark, revisions were slightly more common in sleeve gastrectomy than in gastric bypass (sleeve 0.6%, bypass 0.4%, P = 0.009).
Conclusions and relevance: In a large cohort of commercially insured patients, sleeve gastrectomy had a superior safety profile to gastric bypass up to 2 years from surgery, even when accounting for selection bias. However, the higher risk of revisions in sleeve gastrectomy merits further exploration.
Copyright © 2020 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Campos GM, Khoraki J, Browning MG, Pessoa BM, Mazzini GS, Wolfe L. Changes in Utilization of Bariatric Surgery in the United States From 1993 to 2016. Annals of Surgery. 2019:1. - PubMed
-
- Biter LU, Gadiot RPM, Grotenhuis BA, et al. The Sleeve Bypass Trial: a multicentre randomized controlled trial comparing the long term outcome of laparoscopic sleeve gastrectomy and gastric bypass for morbid obesity in terms of excess BMI loss percentage and quality of life. BMC Obesity. 2015;2(1):30. - PMC - PubMed
-
- Carlin AM, Zeni TM, English WJ, et al. The comparative effectiveness of sleeve gastrectomy, gastric bypass, and adjustable gastric banding procedures for the treatment of morbid obesity. Annals of surgery. 2013;257(5):791–797. - PubMed
-
- Helmio M, Victorzon M, Ovaska J, et al. SLEEVEPASS: a randomized prospective multicenter study comparing laparoscopic sleeve gastrectomy and gastric bypass in the treatment of morbid obesity: preliminary results. Surg Endosc. 2012;26(9):2521–2526. - PubMed
-
- Ignat M, Vix M, Imad I, et al. Randomized trial of Roux-en-Y gastric bypass versus sleeve gastrectomy in achieving excess weight loss. Br J Surg. 2016. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
