

Multicenter International Cohort Validation of a Modified Sequential Organ Failure Assessment Score Using the Richmond Agitation-sedation Scale
- PMID: 33201122
- PMCID: PMC10573707
- DOI: 10.1097/SLA.0000000000004484
Multicenter International Cohort Validation of a Modified Sequential Organ Failure Assessment Score Using the Richmond Agitation-sedation Scale
Abstract
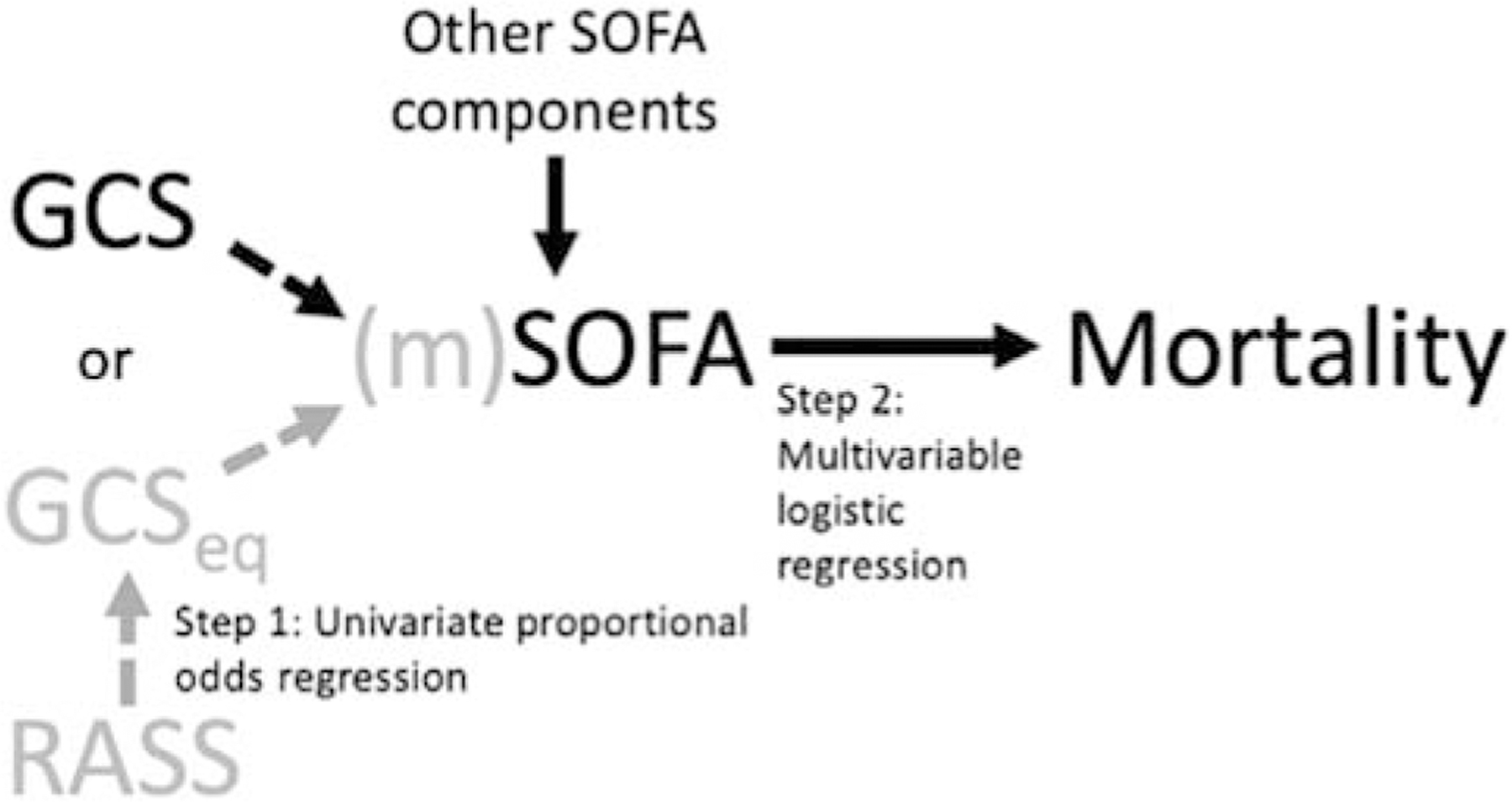
Objective: In a multicenter, international cohort, we aimed to validate a modified Sequential Organ Failure Assessment (mSOFA) using the Richmond Agitation-Sedation Scale, hypothesized as comparable to the Glasgow Coma Scale (GCS)-based Sequential Organ Failure Assessment (SOFA).
Summary background data: The SOFA score, whose neurologic component is based on the GCS, can predict intensive care unit (ICU) mortality. But, GCS is often missing in lieu of other assessments, such as the also reliable and validated Richmond Agitation Sedation Scale (RASS). Single-center data suggested an RASS-based SOFA (mSOFA) predicted ICU mortality.
Methods: Our nested cohort within the prospective 2016 Fourth International Study of Mechanical Ventilation contains 4120 ventilated patients with daily RASS and GCS assessments (20,023 patient-days, 32 countries). We estimated GCS from RASS via a proportional odds model without adjustment. ICU mortality logistic regression models and c-statistics were constructed using SOFA (measured GCS) and mSOFA (measured RASS-estimated GCS), adjusted for age, sex, body-mass index, region (Europe, USA-Canada, Latin America, Africa, Asia, Australia-New Zealand), and postoperative status (medical/surgical).
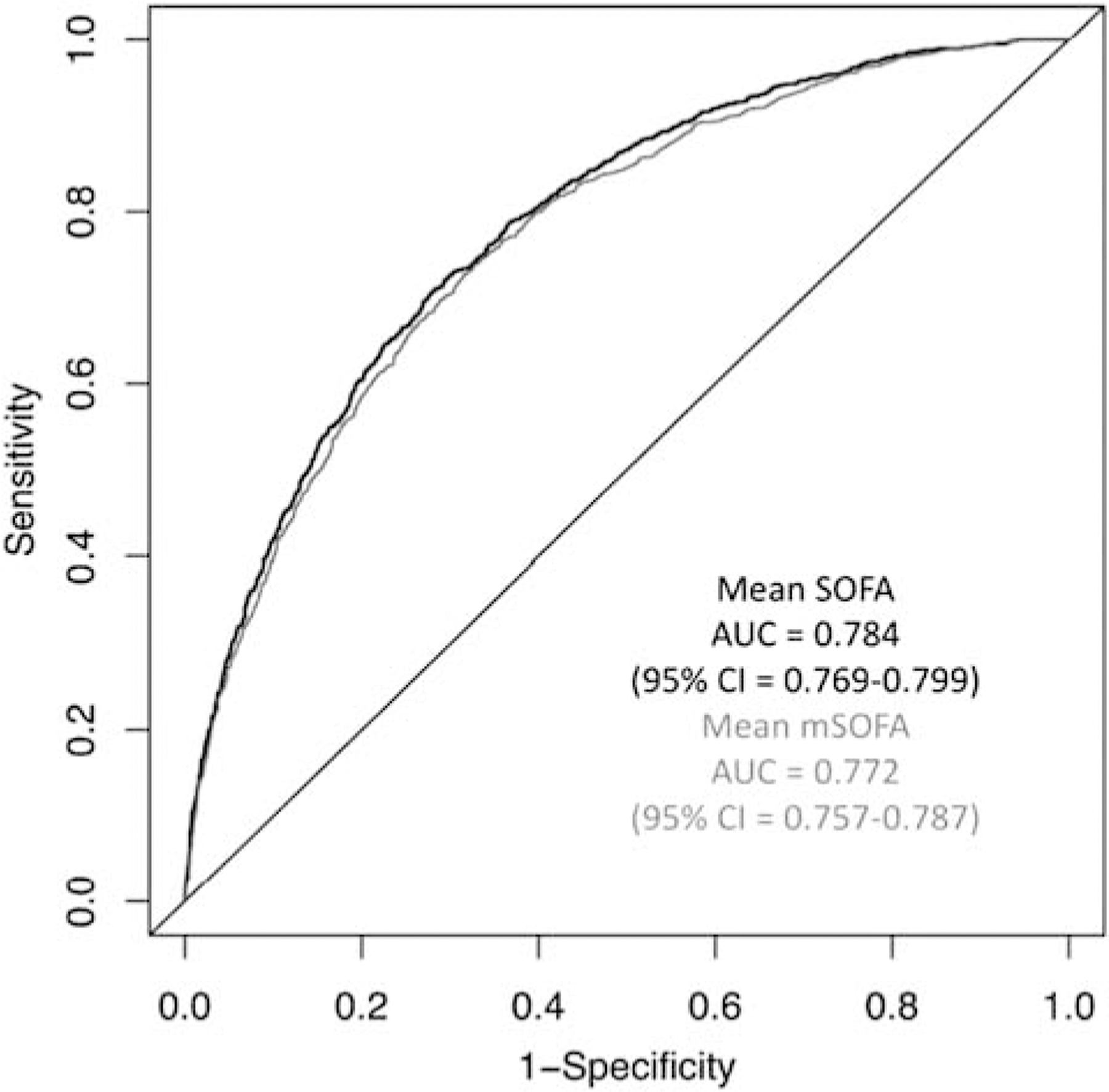
Results: Cohort-wide, the mean SOFA=9.4+/-2.8 and mean mSOFA = 10.0+/-2.3, with ICU mortality = 31%. Mean SOFA and mSOFA similarly predicted ICU mortality (SOFA: AUC = 0.784, 95% CI = 0.769-0.799; mSOFA: AUC = 0.778, 95% CI = 0.763-0.793, P = 0.139). Across models, other predictors of mortality included higher age, female sex, medical patient, and African region (all P < 0.001).
Conclusions: We present the first SOFA modification with RASS in a "real-world" international cohort. Estimating GCS from RASS preserves predictive validity of SOFA to predict ICU mortality. Alternative neurologic measurements like RASS can be viably integrated into severity of illness scoring systems like SOFA.
Copyright © 2020 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no other conflicts of interest.
Figures
References
-
- Vincent J-L, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med 1996;22:707–710. - PubMed
-
- Vincent J-L, Mendonca AD, Cantraine F, et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units. Crit Care Med 1998;26:1793–1800. - PubMed
-
- Ferreira FL, Bota DF, Bross A, et al. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA 2001;286:1754–1758. - PubMed
-
- Nates JL, Cardenas-Turanzas M, Wakefield C, et al. Automating and simplifying the SOFA score in critically ill patients with cancer. Health Informatics J 2010;16:35–47. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
