

Pancreatobiliary Maljunction-associated Gallbladder Cancer Is as Common in the West, Shows Distinct Clinicopathologic Characteristics and Offers an Invaluable Model for Anatomy-induced Reflux-associated Physio-chemical Carcinogenesis
- PMID: 33201123
- PMCID: PMC9305302
- DOI: 10.1097/SLA.0000000000004482
Pancreatobiliary Maljunction-associated Gallbladder Cancer Is as Common in the West, Shows Distinct Clinicopathologic Characteristics and Offers an Invaluable Model for Anatomy-induced Reflux-associated Physio-chemical Carcinogenesis
Abstract
Objective: To determine the associations of pancreatobiliary maljunction (PBM) in the West.
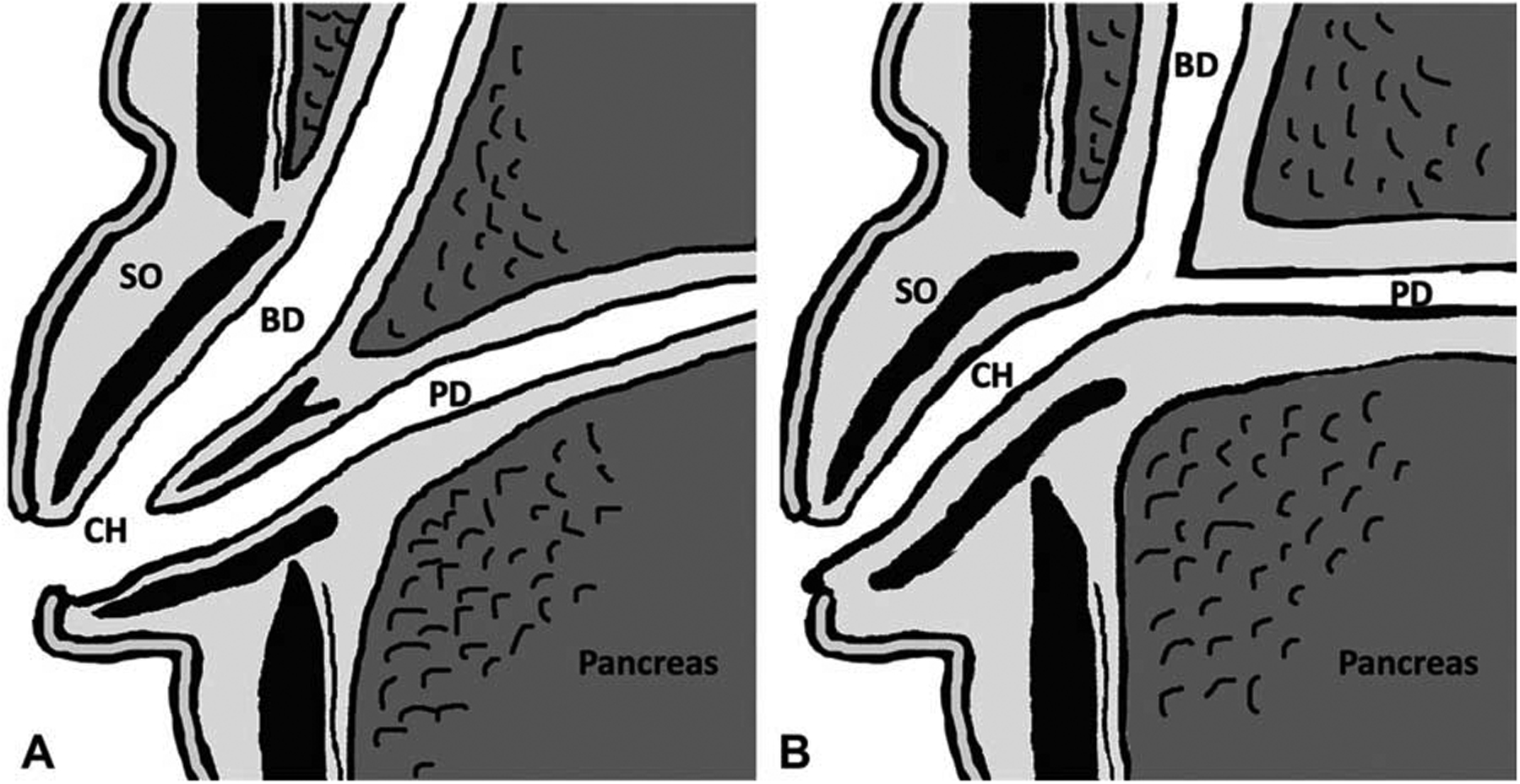
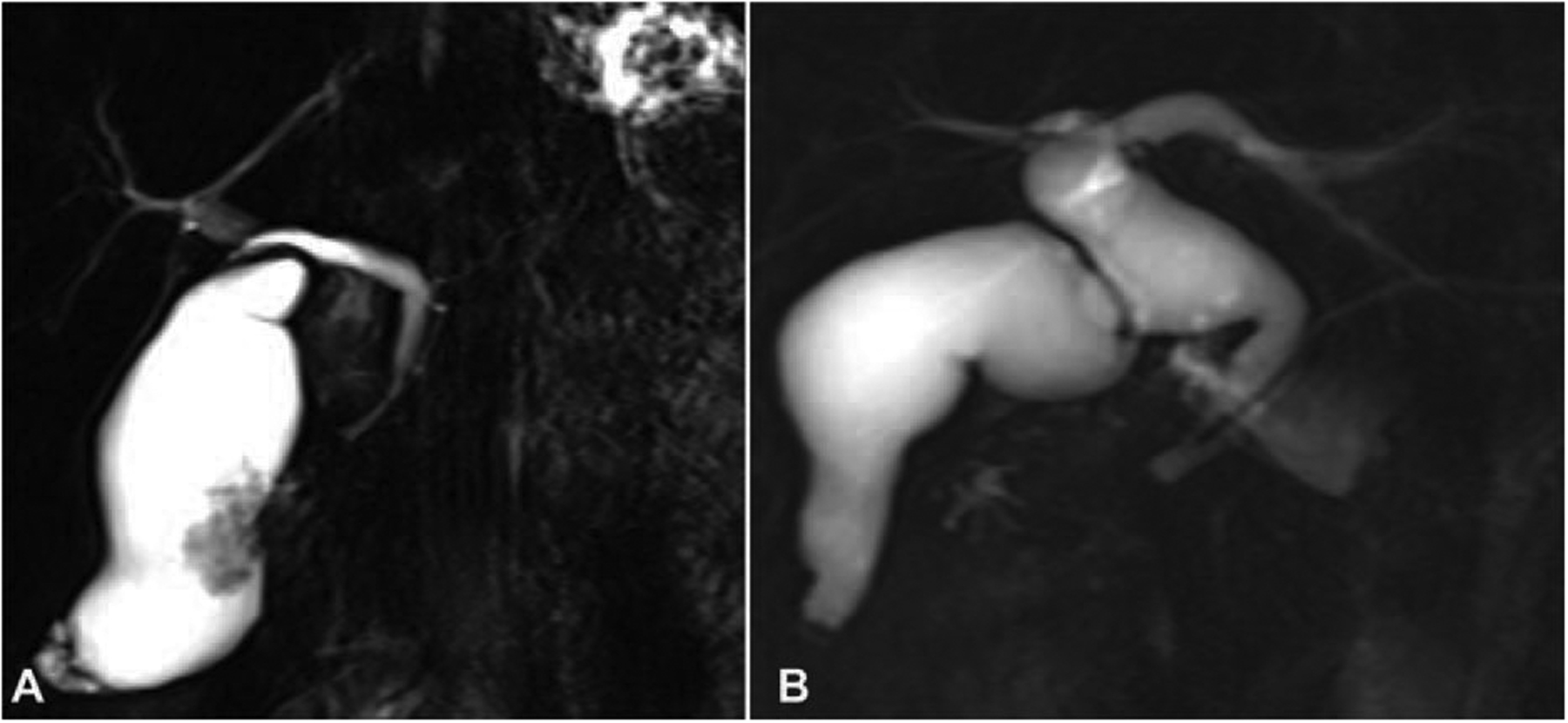
Background: PBM (anomalous union of common bile duct and pancreatic duct) is mostly regarded as an Asian-only disorder, with 200X risk of gallbladder cancer (GBc), attributed to reflux of pancreatic enzymes. Methods: Radiologic images of 840 patients in the US who underwent pancreatobiliary resections were reviewed for PBM and contrasted with 171 GBC cases from Japan.
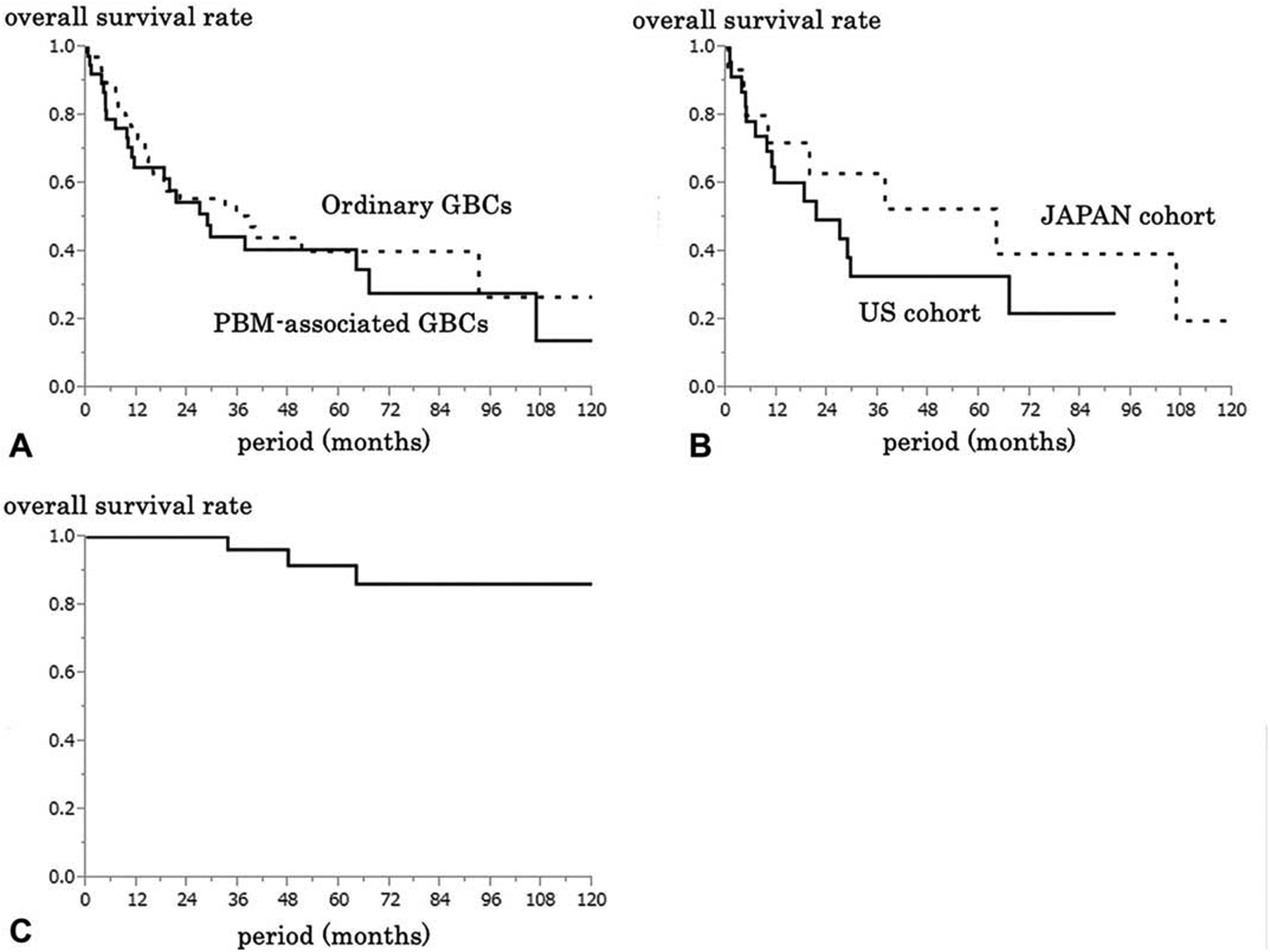
Results: Eight % of the US GBCs (24/300) had PBM (similar to Japan; 15/ 171, 8.8%), in addition to 1/42 bile duct carcinomas and 5/33 choledochal cysts. None of the 30 PBM cases from the US had been diagnosed as PBM in the original work-up. PBM was not found in other pancreatobiliary disorders. Clinicopathologic features of the 39 PBM-associated GBCs (US:24, Japan:15) were similar; however, comparison with non-PBM GBCs revealed that they occurred predominantly in females (F/M = 3); at younger (<50-year-old) age (21% vs 6.5% in non-PBM GBCs; P = 0.01); were uncommonly associated with gallstones (14% vs 58%; P < 0.001); had higher rate of tumor-infiltrating lymphocytes (69% vs 44%; P = 0.04); arose more often through adenoma-carcinoma sequence (31% vs 12%; P = 0.02); and had a higher proportion of nonconventional carcinomas (21% vs 7%; P = 0.03). Conclusions: PBM accounts for 8% of GBCs also in the West but is typically undiagnosed. PBM-GBCs tend to manifest in younger age and often through adenoma-carcinoma sequence, leading to unusual carcinoma types. If PBM is encountered, cholecystectomy and surveillance of bile ducts is warranted. PBM-associated GBCs offer an invaluable model for variant anatomy-induced chemical (reflux-related) carcinogenesis.
Copyright © 2020 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Kozumi K, Kodama T. A case of cystic dilatation of the common bile duct and etiology of the disease (in Japanese). Tokyo Med J. 1916;30:1413–1423.
-
- Babbitt DP. Congenital choledochal cysts: new etiological concept based on anomalous relationships of the common bile duct and pancreatic bulb. Ann Radiol (Paris). 1969;12:231–240. - PubMed
-
- Komi N, Kuwashima T, Kuramoto M, et al. Anomalous arrangement of the pancreaticobiliary ductal system in choledochal cyst. Tokushima J Exp Med. 1976;23:37–48. - PubMed
-
- The Japanese Study Group on Pancreaticobiliary Maljunction (JSGPM). Committee for Diagnostic Criteria for Pancreaticobiliary Maljunction. Diagnostic criteria of pancreaticobiliary maljunction (in Japanese). Tan to Sui. 1987;8:115–118.
-
- The Japanese Study Group on Pancreaticobiliary Maljunction (JSPBM). The Committee of JSPBM for Diagnostic Criteria. Diagnostic criteria of pancreaticobiliary maljunction. J Hepatobiliary Pancreat Surg. 1994;1:219–221.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
