

Evaluation of a Patient-Centered Fall-Prevention Tool Kit to Reduce Falls and Injuries: A Nonrandomized Controlled Trial
- PMID: 33201236
- PMCID: PMC7672520
- DOI: 10.1001/jamanetworkopen.2020.25889
Evaluation of a Patient-Centered Fall-Prevention Tool Kit to Reduce Falls and Injuries: A Nonrandomized Controlled Trial
Abstract
Importance: Falls represent a leading cause of preventable injury in hospitals and a frequently reported serious adverse event. Hospitalization is associated with an increased risk for falls and serious injuries including hip fractures, subdural hematomas, or even death. Multifactorial strategies have been shown to reduce falls in acute care hospitals, but evidence for fall-related injury prevention in hospitals is lacking.
Objective: To assess whether a fall-prevention tool kit that engages patients and families in the fall-prevention process throughout hospitalization is associated with reduced falls and injurious falls.
Design, setting, and participants: This nonrandomized controlled trial using stepped wedge design was conducted between November 1, 2015, and October 31, 2018, in 14 medical units within 3 academic medical centers in Boston and New York City. All adult inpatients hospitalized in participating units were included in the analysis.
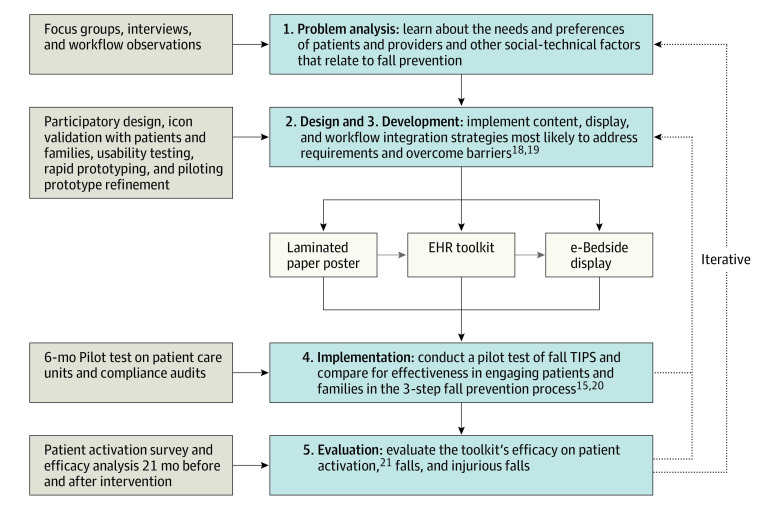
Interventions: A nurse-led fall-prevention tool kit linking evidence-based preventive interventions to patient-specific fall risk factors and designed to integrate continuous patient and family engagement in the fall-prevention process.
Main outcomes and measures: The primary outcome was the rate of patient falls per 1000 patient-days in targeted units during the study period. The secondary outcome was the rate of falls with injury per 1000 patient-days.
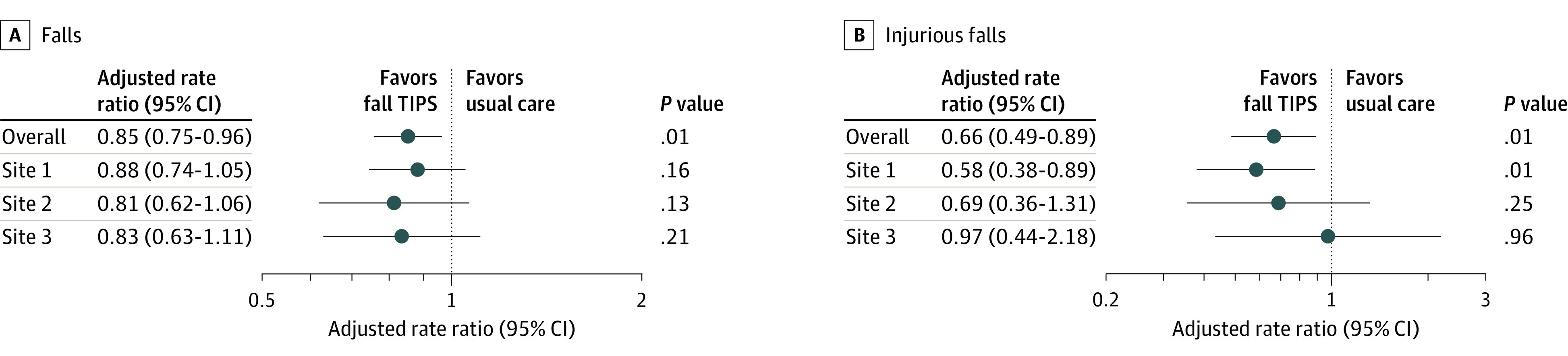
Results: During the interrupted time series, 37 231 patients were evaluated, including 17 948 before the intervention (mean [SD] age, 60.56 [18.30] years; 9723 [54.17%] women) and 19 283 after the intervention (mean [SD] age, 60.92 [18.10] years; 10 325 [53.54%] women). There was an overall adjusted 15% reduction in falls after implementation of the fall-prevention tool kit compared with before implementation (2.92 vs 2.49 falls per 1000 patient-days [95% CI, 2.06-3.00 falls per 1000 patient-days]; adjusted rate ratio 0.85; 95% CI, 0.75-0.96; P = .01) and an adjusted 34% reduction in injurious falls (0.73 vs 0.48 injurious falls per 1000 patient-days [95% CI, 0.34-0.70 injurious falls per 1000 patient-days]; adjusted rate ratio, 0.66; 95% CI, 0.53-0.88; P = .003).
Conclusions and relevance: In this nonrandomized controlled trial, implementation of a fall-prevention tool kit was associated with a significant reduction in falls and related injuries. A patient-care team partnership appears to be beneficial for prevention of falls and fall-related injuries.
Trial registration: ClinicalTrials.gov Identifier: NCT02969343.
Conflict of interest statement
Figures

References
-
- Serious reportable events National Quality Forum. in healthcare: 2011 update. Published 2011. Accessed October 12, 2020. http://www.qualityforum.org/topics/sres/serious_reportable_events.aspx
-
- Centers for Disease Control and Prevention WISQARS—Web-based Injury Statistics Query and Reporting System. Updated July 1, 2020. Accessed October 7, 2020. https://www.cdc.gov/injury/wisqars/index.html
