

The role for high flow nasal cannula as a respiratory support strategy in adults: a clinical practice guideline
- PMID: 33201321
- PMCID: PMC7670292
- DOI: 10.1007/s00134-020-06312-y
The role for high flow nasal cannula as a respiratory support strategy in adults: a clinical practice guideline
Abstract
Purpose: High flow nasal cannula (HFNC) is a relatively recent respiratory support technique which delivers high flow, heated and humidified controlled concentration of oxygen via the nasal route. Recently, its use has increased for a variety of clinical indications. To guide clinical practice, we developed evidence-based recommendations regarding use of HFNC in various clinical settings.
Methods: We formed a guideline panel composed of clinicians, methodologists and experts in respiratory medicine. Using GRADE, the panel developed recommendations for four actionable questions.
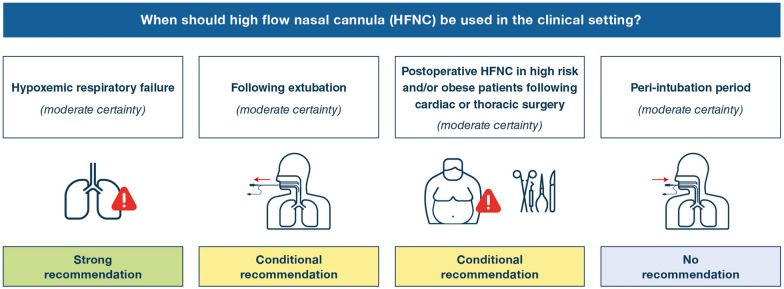
Results: The guideline panel made a strong recommendation for HFNC in hypoxemic respiratory failure compared to conventional oxygen therapy (COT) (moderate certainty), a conditional recommendation for HFNC following extubation (moderate certainty), no recommendation regarding HFNC in the peri-intubation period (moderate certainty), and a conditional recommendation for postoperative HFNC in high risk and/or obese patients following cardiac or thoracic surgery (moderate certainty).
Conclusions: This clinical practice guideline synthesizes current best-evidence into four recommendations for HFNC use in patients with hypoxemic respiratory failure, following extubation, in the peri-intubation period, and postoperatively for bedside clinicians.
Keywords: Extubation; High flow nasal cannula; Mortality; Peri-intubation; Postoperative; Respiratory failure.
Conflict of interest statement
SE received funding for travel, given lectures, owns patents with and/or performed consultancy work for Zoll, Medtronic and Diasorin and has participated in multicentre trials run by Artisanpharma, Eisai and Astra Zeneca. JM received personal fees from Faron Pharmaceuticals, Medtronic and Janssen; IMT Medical provided travel and hotel expenses to attend a meeting; he is a coinvestigator on a PAV + multinational trial funded by the CIHR in partnership with Covidien (Medtronic); more than 3 years ago Fisher-Paykel, General Electric and A-Lung provided grant funding to conduct clinical research. TM received lecture fees from Drager, Fisher and Paykel, Mindray and BBraun. EG supported by an Early Career Investigator award from the Canadian Institutes of Health Research. He receives financial and nonfinancial support from Getinge and Timpel outside the submitted work. SJ received Consulting fees from Drager, Xenios, and Fisher & Paykel. J-DR received travel expenses and accommodation coverage from Fisher&Paykel Healthcare to attend scientific meetings. Fisher&Paykel Healthcare provided support for the ongoing High Flow ACRF trial (NCT03406572) but took no part in design or conduct of the study. NR received travel expenses and lecture fees from Fisher&Paykel. OR’s institution received fees for consultation from Hamilton Medical and received lecture fees from Air Liquide. MA’s institution received unrestricted research grant from Fisher & Paykel and GE Healthcare, he received consulting fees from Getinge and Intersurgical. SMM received consulting fees from Draeger Medical and General Electric Healthcare; his Institution received a research grant from Fisher and Paykel Healthcare (the RINO trial,
References
-
- Nishimura M. High-flow nasal cannula oxygen therapy in adults: physiological benefits, indication, clinical benefits, and adverse effects. Respir Care. 2016;61(4):529–541. - PubMed
-
- Papazian L, Corley A, Hess D, et al. Use of high-flow nasal cannula oxygenation in ICU adults: a narrative review. Intensive Care Med. 2016;42(9):1336–1349. - PubMed
-
- Ito J, Nagata K, Sato S, et al. The clinical practice of high-flow nasal cannula oxygen therapy in adults: a Japanese cross-sectional multicenter survey. Respir Investig. 2018;56(3):249–257. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
