

Adverse Effects of Low-Dose Methotrexate in a Randomized Double-Blind Placebo-Controlled Trial: Adjudicated Hematologic and Skin Cancer Outcomes in the Cardiovascular Inflammation Reduction Trial
- PMID: 33201596
- PMCID: PMC7738806
- DOI: 10.1002/acr2.11187
Adverse Effects of Low-Dose Methotrexate in a Randomized Double-Blind Placebo-Controlled Trial: Adjudicated Hematologic and Skin Cancer Outcomes in the Cardiovascular Inflammation Reduction Trial
Abstract
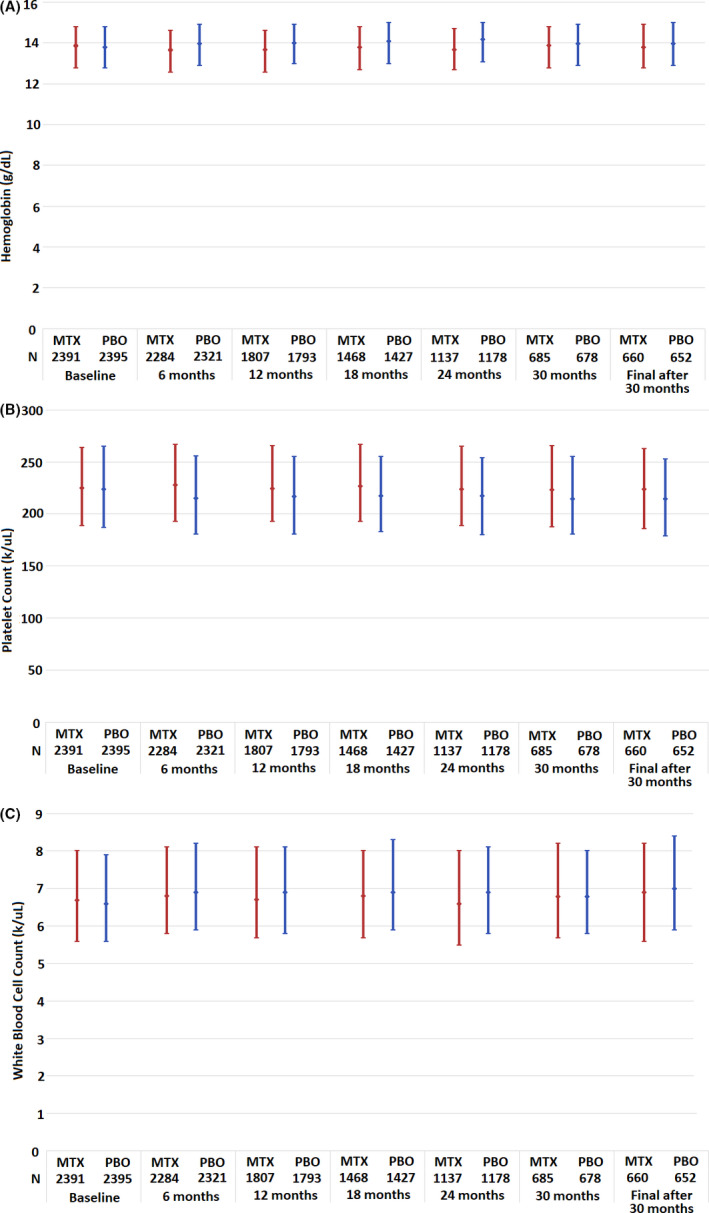
Objective: Low-dose methotrexate (LD-MTX), a cornerstone in the treatment of rheumatoid arthritis, is associated with a moderately increased risk of anemia, leukopenia, and skin cancers, but the risks of myelosuppression and malignancy during LD-MTX use remain incompletely described. We examined the risks of cytopenias and skin cancers among patients taking LD-MTX versus placebo in a large randomized controlled trial (RCT).
Methods: We prespecified secondary analyses of a double-blind, placebo-controlled RCT that included adults with known cardiovascular disease and diabetes or metabolic syndrome in the United States and Canada. Subjects were randomly allocated to LD-MTX (20 mg/week maximum) or placebo. All subjects received folic acid (1 mg daily for 6days/week). We assessed the frequency of blindly adjudicated hematologic and malignant adverse events (AEs).
Results: A total of 2391 subjects were randomized to LD-MTX (mean dosage 14.9 mg/week), and 2395 were randomized to placebo. During follow-up, in the LD-MTX arm, simultaneous two-line cytopenias (n = 92 [3.9%]) or pancytopenia (n = 13 [0.54%]) were infrequent. Pancytopenia developed as soon as 4 months and as late as 3.5 years after beginning LD-MTX, though the latter subject had been recently diagnosed with multiple myeloma. Overall skin cancer risk was increased in users of LD-MTX compared with users of placebo, which driven largely by a statistically significant increased risk of squamous cell skin cancer (hazard ratio [HR] 3.31; 95% confidence interval [CI] 1.63-6.71). Melanoma was increased in LD-MTX, but this was not statistically significant (HR 2.33; 95% CI 0.60-9.01).
Conclusions: Among subjects using LD-MTX, simultaneous two-line cytopenias and pancytopenia were uncommon. We found more cases of skin cancer, particularly squamous cell carcinomas, in the LD-MTX arm than the placebo arm.
© 2020 The Authors. ACR Open Rheumatology published by Wiley Periodicals LLC on behalf of American College of Rheumatology.
Figures
References
-
- Farber S, Diamond LK. Temporary remissions in acute leukemia in children produced by folic acid antagonist, 4‐aminopteroyl‐glutamic acid. N Engl J Med 1948;238:787–93. - PubMed
-
- Gutierrez‐Ureña S, Molina JF, García CO, Cuéllar ML, Espinoza LR. Pancytopenia secondary to methotrexate therapy in rheumatoid arthritis. Arthritis Rheum 1996;39:272–6. - PubMed
-
- Williams HJ, Willkens RF, Samuelson CO, Alarcón GS, Guttadauria M, Yarboro C, et al. Comparison of low‐dose oral pulse methotrexate and placebo in the treatment of rheumatoid arthritis. Arthritis Rheum 1985;28:721–30. - PubMed
-
- Van Ede AE, Laan RF, Rood MJ, Huizinga TW, van de Laar MA, van Denderen CJ, et al. Effect of folic or folinic acid supplementation on the toxicity and efficacy of methotrexate in rheumatoid arthritis: a forty‐eight week, multicenter, randomized, double‐blind, placebo‐controlled study. Arthritis Rheum 2001;44:1515–24. - PubMed
-
- Solomon DH, Kremer JM, Fisher M, Curtis JR, Furer V, Harrold LR, et al. Comparative cancer risk associated with methotrexate, other non‐biologic and biologic disease‐modifying anti‐rheumatic drugs. Semin Arthritis Rheum 2014;43:489–97. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
