

Accuracy of high-resolution ultrasound (US) for gingival soft tissue thickness mesurement in edentulous patients prior to implant placement
- PMID: 33201732
- PMCID: PMC8231686
- DOI: 10.1259/dmfr.20200309
Accuracy of high-resolution ultrasound (US) for gingival soft tissue thickness mesurement in edentulous patients prior to implant placement
Abstract
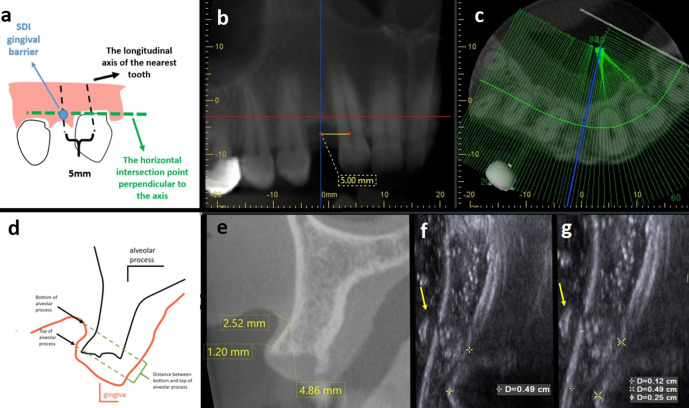
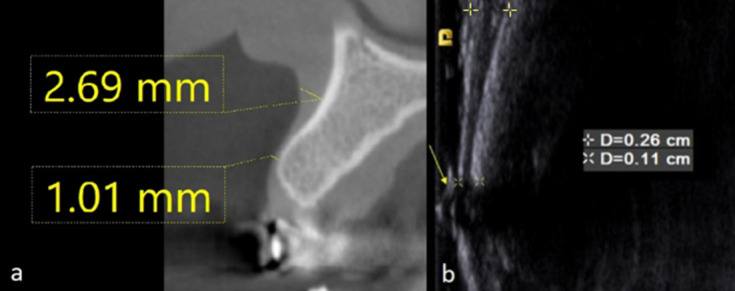
Objectives: To evaluate and compare the accuracy of high-resolution ultrasound (US) with two different cone beam CT (CBCT) units and clinical assessment for measuring gingival soft tissue thickness in edentulous patients prior to implant placement.
Methods and materials: The study consisted of 40 maxillary implant sites of 40 healthy patients (20 females, 20 males; mean age, 47.88 years). We prospectively evaluated labial/buccal gingival thickness in 40 implant regions (16 anterior and 24 posterior) by using limited field of view (FOV) CBCT images and US images in comparison to gold standard transgingival probing measurements. One-way analysis of variance (ANOVA) was used to compare mean measurements obtained from CBCT (Morita and Planmeca), US, and transgingival probing. Interclass correlation coefficient (ICC) estimates were calculated based on means with two-way mixed and absolute-agreement model. Bland Altman plot was used to describe agreement between clinical vs US and CBCT measurements by constructing limits of agreement. Statistical significance was set at p < 0.05.
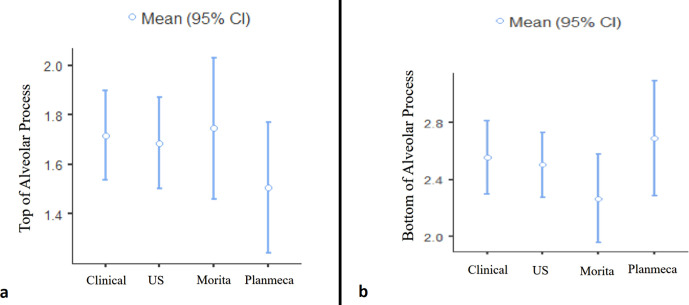
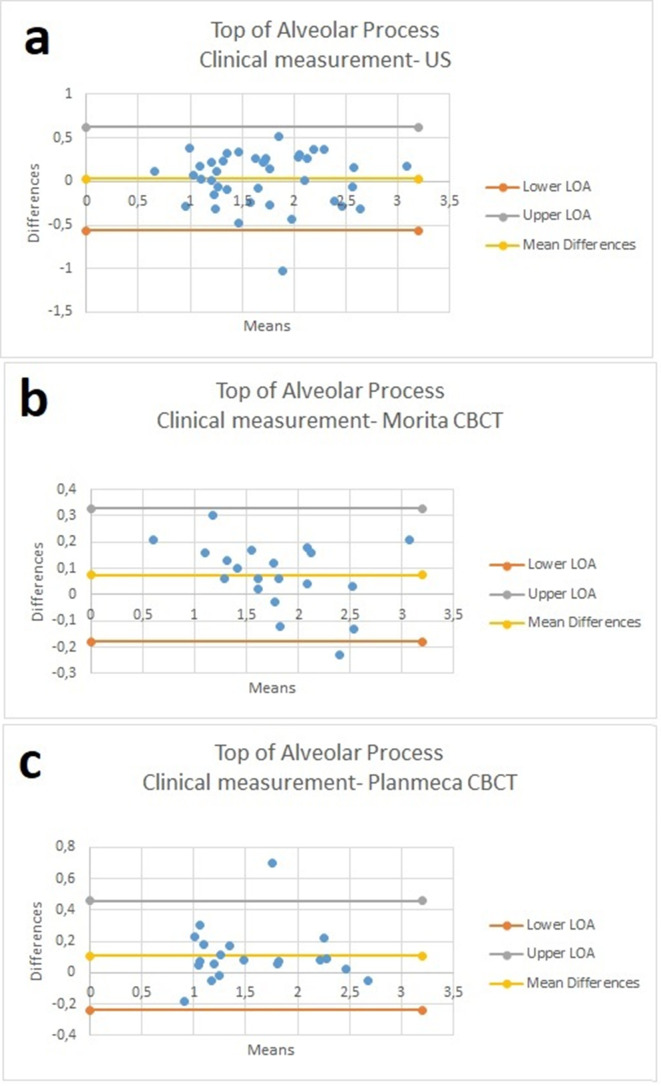
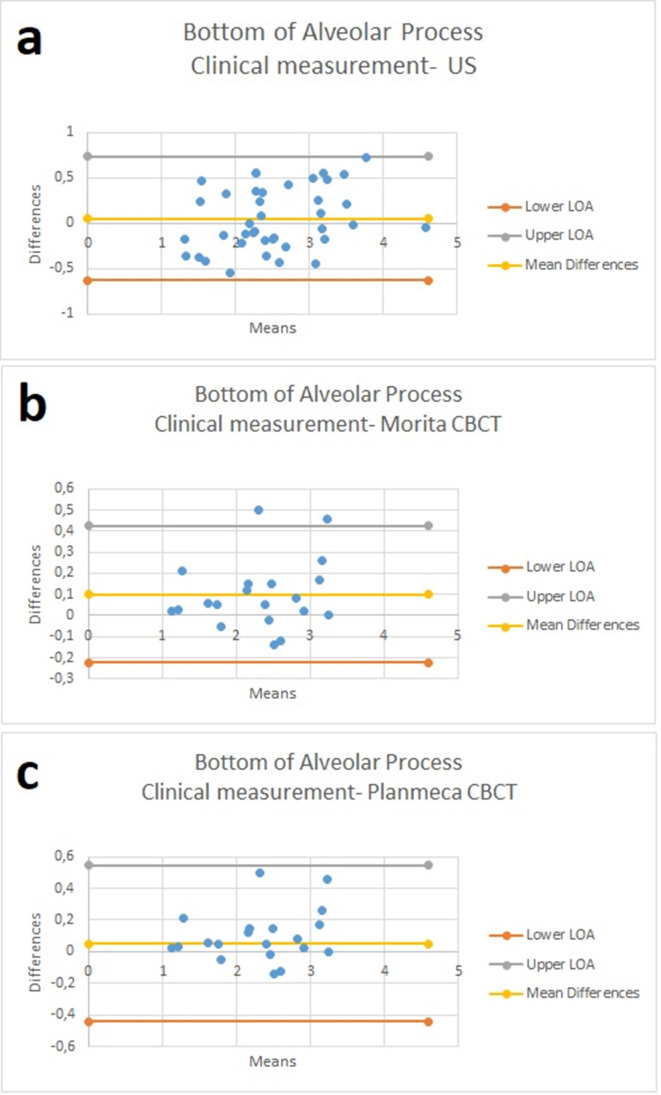
Results: There was no significant difference between methods used according to mean gingival thickness measurements obtained from the top (p = 0.519) and bottom (p = 0.346) of the alveolar process. US and CBCT measurements highly correlated with clinical measurements for both top and bottom alveolar process gingival thickness (p < 0.001). Distribution of differences between clinical measurements and both CBCT measurements showed statistically significant differences according to 0 (p < 0.05). Distribution of differences between clinical measurements and US measurements did not show statistically significant difference (p > 0.05).
Conclusion: High-resolution US provided accurate information for the measurement of gingival soft tissue thickness in edentulous patients prior to implant placement.
Keywords: Dental implantation; Gingival thickness; Measurement; Ultrasonography.
Figures

References
-
- Levin L, Pathael S, Dolev E, Schwartz-Arad D. Aesthetic versus surgical success of single dental implants: 1- to 9-year follow-up. Pract Proced Aesthet Dent 2005; 17: 533–8. - PubMed
-
- Cook DR, Mealey BL, Verrett RG, Mills MP, Noujeim ME, Lasho DJ, et al. Relationship between clinical periodontal biotype and labial plate thickness: an in vivo study. Int J Periodontics Restorative Dent 2011; 31: 345–54. - PubMed
-
- Fu J-H, Lee A, Wang H-L. Influence of tissue biotype on implant esthetics. Int J Oral Maxillofac Implants 2011; 26: 499–508. - PubMed
