

Clinical, regional, and genetic characteristics of Covid-19 patients from UK Biobank
- PMID: 33201886
- PMCID: PMC7671499
- DOI: 10.1371/journal.pone.0241264
Clinical, regional, and genetic characteristics of Covid-19 patients from UK Biobank
Abstract
Background: Coronavirus disease 2019 (Covid-19) has rapidly infected millions of people worldwide. Recent studies suggest that racial minorities and patients with comorbidities are at higher risk of Covid-19. In this study, we analyzed the effects of clinical, regional, and genetic factors on Covid-19 positive status.
Methods: The UK Biobank is a longitudinal cohort study that recruited participants from 2006 to 2010 from throughout the United Kingdom. Covid-19 test results were provided to UK Biobank starting on March 16, 2020. The main outcome measure in this study was Covid-19 positive status, determined by the presence of any positive test for a single individual. Clinical risk factors were derived from UK Biobank at baseline, and regional risk factors were imputed using census features local to each participant's home zone. We used robust adjusted Poisson regression with clustering by testing laboratory to estimate relative risk. Blood types were derived using genetic variants rs8176719 and rs8176746, and genomewide tests of association were conducted using logistic-Firth hybrid regression.
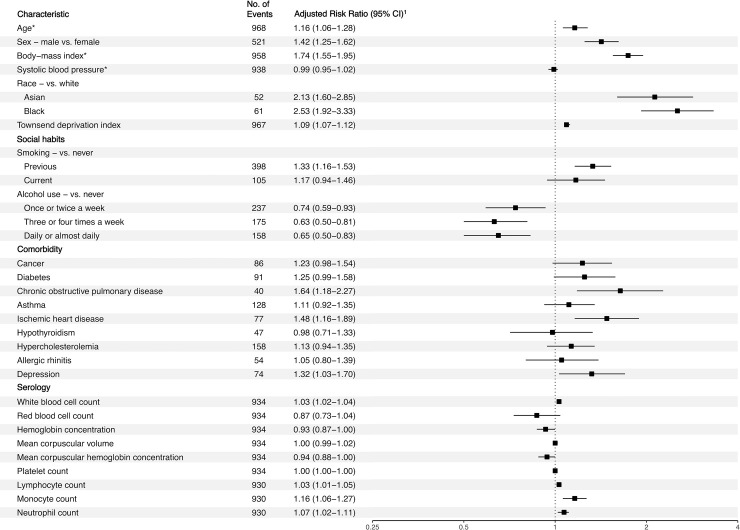
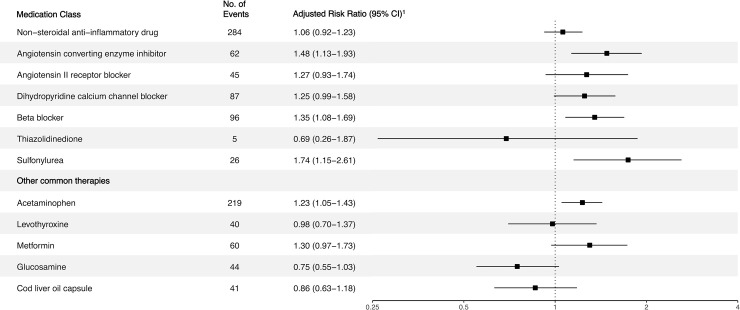
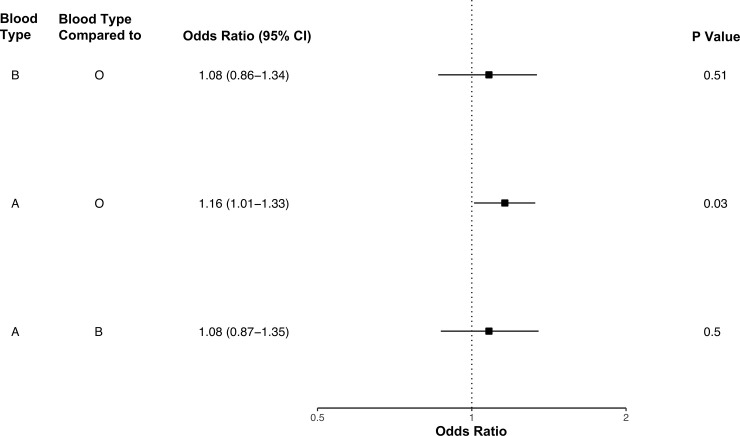
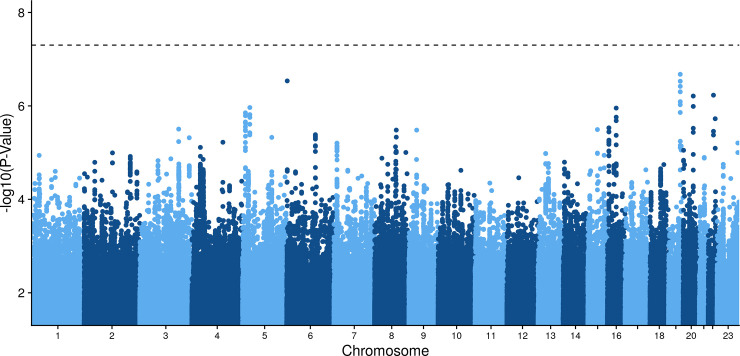
Results: This prospective cohort study included 397,064 UK Biobank participants, of whom 968 tested positive for Covid-19. The unadjusted relative risk of Covid-19 for Black participants was 3.66 (95% CI 2.83-4.74), compared to White participants. Adjusting for Townsend deprivation index alone reduced the relative risk to 2.44 (95% CI 1.86-3.20). Comorbidities that significantly increased Covid-19 risk included chronic obstructive pulmonary disease (adjusted relative risk [ARR] 1.64, 95% CI 1.18-2.27), ischemic heart disease (ARR 1.48, 95% CI 1.16-1.89), and depression (ARR 1.32, 95% CI 1.03-1.70). There was some evidence that angiotensin converting enzyme inhibitors (ARR 1.48, 95% CI 1.13-1.93) were associated with increased risk of Covid-19. Each standard deviation increase in the number of total individuals living in a participant's locality was associated with increased risk of Covid-19 (ARR 1.14, 95% CI 1.08-1.20). Analyses of genetically inferred blood types confirmed that participants with type A blood had increased odds of Covid-19 compared to participants with type O blood (odds ratio [OR] 1.16, 95% CI 1.01-1.33). A meta-analysis of genomewide association studies across ancestry groups did not reveal any significant loci. Study limitations include confounding by indication, bias due to limited information on early Covid-19 test results, and inability to accurately gauge disease severity.
Conclusions: When assessing the association of Black race with Covid-19, adjusting for deprivation reduced the relative risk of Covid-19 by 33%. In the context of sociological research, these findings suggest that discrimination in the labor market may play a role in the high relative risk of Covid-19 for Black individuals. In this study, we also confirmed the association of blood type A with Covid-19, among other clinical and regional factors.
Conflict of interest statement
OE reports grants from the National Institutes of Health and the Emerson Research Collective. The funders had no role in any aspect of study design, analysis, writing, or other aspects related to the submitted work. There are no relationships or activities that have influenced the submitted work. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Update of
-
Clinical and Genetic Characteristics of Covid-19 Patients from UK Biobank.medRxiv [Preprint]. 2020 May 5:2020.05.05.20075507. doi: 10.1101/2020.05.05.20075507. medRxiv. 2020. Update in: PLoS One. 2020 Nov 17;15(11):e0241264. doi: 10.1371/journal.pone.0241264. PMID: 32511589 Free PMC article. Updated. Preprint.
References
-
- COVID-19 in Racial and Ethnic Minority Groups. Centers for Disease Control and Prevention. 2020.
-
- Coronavirus (COVID-19) related deaths by ethnic group, England and Wales: 2 March 2020 to 10 April 2020. Office for National Statistics. 2020. Available: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarri...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
