

Distal organ inflammation and injury after resuscitative endovascular balloon occlusion of the aorta in a porcine model of severe hemorrhagic shock
- PMID: 33201908
- PMCID: PMC7671515
- DOI: 10.1371/journal.pone.0242450
Distal organ inflammation and injury after resuscitative endovascular balloon occlusion of the aorta in a porcine model of severe hemorrhagic shock
Abstract
Background and objective: Resuscitative Endovascular Balloon Occlusion of Aorta (REBOA) has emerged as a potential life-saving maneuver for the management of non-compressible torso hemorrhage in trauma patients. Complete REBOA (cREBOA) is inherently associated with the burden of ischemia reperfusion injury (IRI) and organ dysfunction. However, the distal organ inflammation and its association with organ injury have been little investigated. This study was conducted to assess these adverse effects of cREBOA following massive hemorrhage in swine.
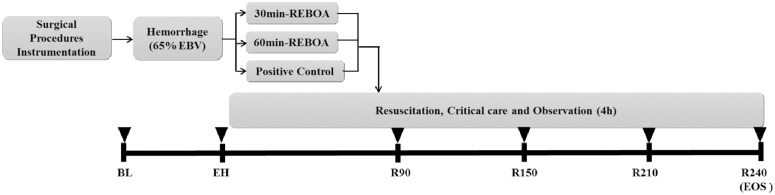
Methods: Spontaneously breathing and consciously sedated Sinclair pigs were subjected to exponential hemorrhage of 65% total blood volume over 60 minutes. Animals were randomized into 3 groups (n = 7): (1) Positive control (PC) received immediate transfusion of shed blood after hemorrhage, (2) 30min-cREBOA (A30) received Zone 1 cREBOA for 30 minutes, and (3) 60min-cREBOA (A60) given Zone 1 cREBOA for 60 minutes. The A30 and A60 groups were followed by resuscitation with shed blood post-cREBOA and observed for 4h. Metabolic and hemodynamic effects, coagulation parameters, inflammatory and end organ consequences were monitored and assessed.
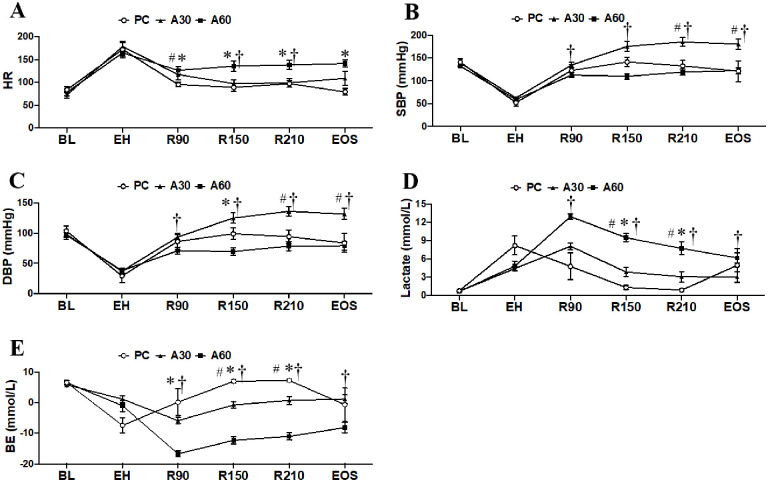
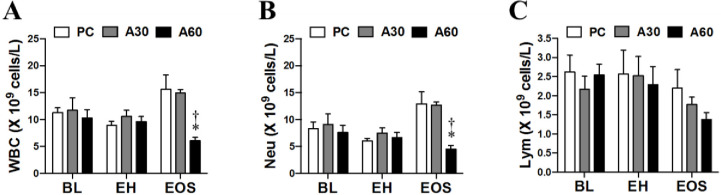
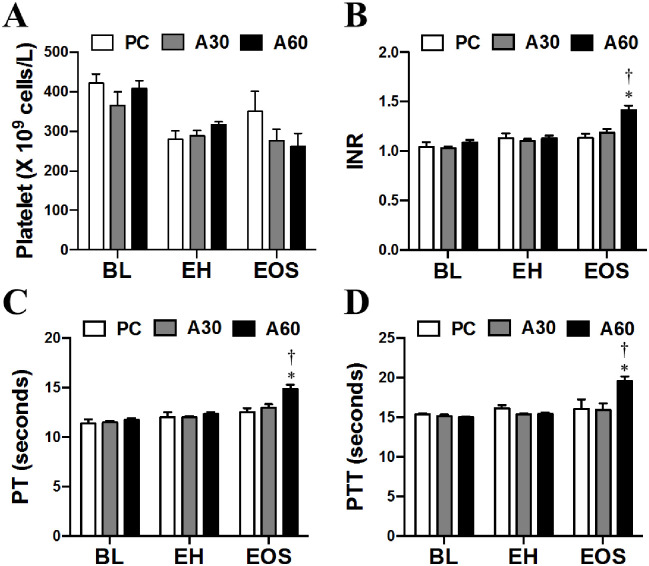
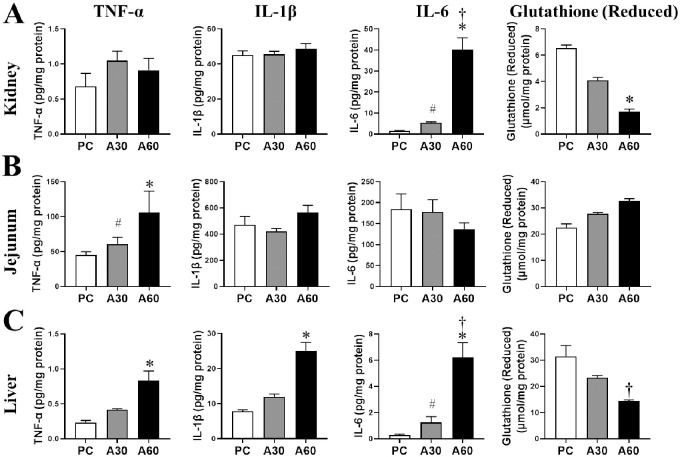
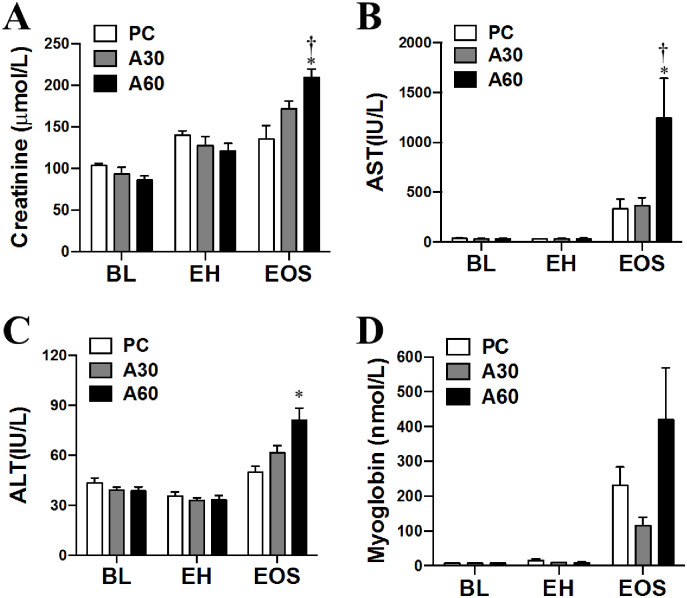
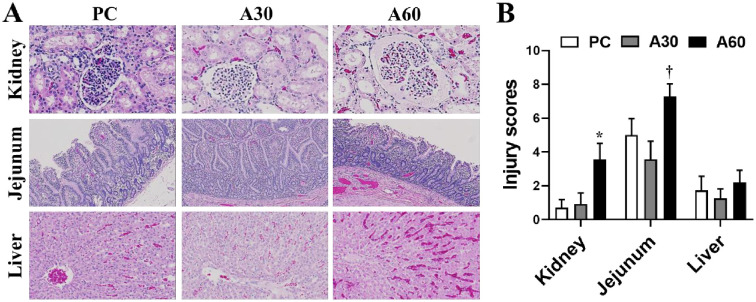
Results: Compared with 30min-cREBOA, 60min-cREBOA resulted in (1) increased IL-6, TNF-α, and IL-1β in distal organs (kidney, jejunum, and liver) (p < 0.05) and decreased reduced glutathione in kidney and liver (p < 0.05), (2) leukopenia, neutropenia, and coagulopathy (p < 0.05), (3) blood pressure decline (p < 0.05), (4) metabolic acidosis and hyperkalemia (p < 0.05), and (5) histological injury of kidney and jejunum (p < 0.05) as well as higher levels of creatinine, AST, and ALT (p < 0.05).
Conclusion: 30min-cREBOA seems to be a feasible and effective adjunct in supporting central perfusion during severe hemorrhage. However, prolonged cREBOA (60min) adverse effects such as distal organ inflammation and injury must be taken into serious consideration.
Conflict of interest statement
The authors declare that they have no conflicts of interest relevant to the manuscript. Although this research was funded partially by a subcontract between Prytime Medical and the Geneva Foundation, Tacoma, WA, for the work performed at the US Army Institute of Surgical Research, the commercial founder had no role in study design, data collection, analysis and interpretation, decision to publish, or preparation of the manuscript. This also does not alter our adherence to PLOS ONE policies on sharing data and materials. None of authors served as a consultant or a board member, participated in their patent and grants application, and received stock, share or travel funds from the commercial founders.
Figures
Similar articles
-
Efficacy of partial and complete resuscitative endovascular balloon occlusion of the aorta in the hemorrhagic shock model of liver injury.World J Emerg Med. 2024;15(1):10-15. doi: 10.5847/wjem.j.1920-8642.2024.001. World J Emerg Med. 2024. PMID: 38188550 Free PMC article.
-
Intermittent thoracic resuscitative endovascular balloon occlusion of the aorta improves renal function compared to 60 min continuous application after porcine class III hemorrhage.Eur J Trauma Emerg Surg. 2023 Jun;49(3):1303-1313. doi: 10.1007/s00068-022-02189-2. Epub 2022 Dec 5. Eur J Trauma Emerg Surg. 2023. PMID: 36471055 Free PMC article.
-
Use of resuscitative endovascular balloon occlusion of the aorta in a highly lethal model of noncompressible torso hemorrhage.Shock. 2014 Feb;41(2):130-7. doi: 10.1097/SHK.0000000000000085. Shock. 2014. PMID: 24430492
-
Resuscitative endovascular balloon occlusion of the aorta.Resuscitation. 2015 Nov;96:275-9. doi: 10.1016/j.resuscitation.2015.09.003. Epub 2015 Sep 16. Resuscitation. 2015. PMID: 26386370 Review.
-
Partial Resuscitative Endovascular Balloon Occlusion of the Aorta: A Systematic Review of the Preclinical and Clinical Literature.J Surg Res. 2021 Jun;262:101-114. doi: 10.1016/j.jss.2020.12.054. Epub 2021 Feb 6. J Surg Res. 2021. PMID: 33561721
Cited by
-
Resuscitative endovascular balloon occlusion of the aorta in combat casualties: The past, present, and future.J Trauma Acute Care Surg. 2021 Aug 1;91(2S Suppl 2):S56-S64. doi: 10.1097/TA.0000000000003166. J Trauma Acute Care Surg. 2021. PMID: 33797487 Free PMC article. Review.
-
INVESTIGATING THE RELATIONSHIP BETWEEN BLEEDING, CLOTTING, AND COAGULOPATHY DURING AUTOMATED PARTIAL REBOA STRATEGIES IN A HIGHLY LETHAL PORCINE HEMORRHAGE MODEL.Shock. 2024 Aug 1;62(2):265-274. doi: 10.1097/SHK.0000000000002385. Epub 2024 Jun 11. Shock. 2024. PMID: 38888571 Free PMC article.
-
A modified chain-based sponge dressing controls junctional hemorrhage in the tactical combat casualty care simulation of pigs.Scand J Trauma Resusc Emerg Med. 2023 Nov 9;31(1):75. doi: 10.1186/s13049-023-01133-6. Scand J Trauma Resusc Emerg Med. 2023. PMID: 37946246 Free PMC article.
-
Efficacy of partial and complete resuscitative endovascular balloon occlusion of the aorta in the hemorrhagic shock model of liver injury.World J Emerg Med. 2024;15(1):10-15. doi: 10.5847/wjem.j.1920-8642.2024.001. World J Emerg Med. 2024. PMID: 38188550 Free PMC article.
-
CORM-3 alleviates the intestinal injury in a rodent model of hemorrhage shock and resuscitation: roles of GFAP-positive glia.J Mol Histol. 2023 Aug;54(4):271-282. doi: 10.1007/s10735-023-10133-w. Epub 2023 Jun 19. J Mol Histol. 2023. PMID: 37335421
References
-
- Butler FK Jr., Holcomb JB, Shackelford S, Barbabella S, Bailey JA, Baker JB, et al. Advanced Resuscitative Care in Tactical Combat Casualty Care: TCCC Guidelines Change 18–01:14 October 2018. J Spec Oper Med. 18(4):37–55. . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
