

Clinical practice guidelines: Oral health care for children and adults living with epidermolysis bullosa
- PMID: 33202040
- PMCID: PMC7756753
- DOI: 10.1111/scd.12511
Clinical practice guidelines: Oral health care for children and adults living with epidermolysis bullosa
Abstract
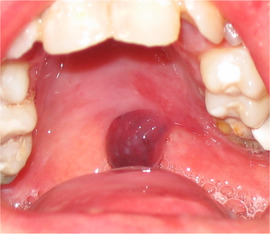
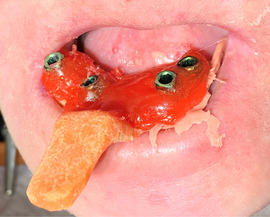
Background: Inherited epidermolysis bullosa (EB) is a genetic disorder characterized by skin fragility and unique oral features.
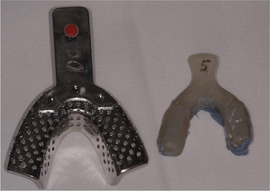
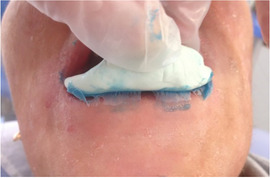
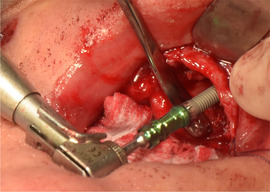
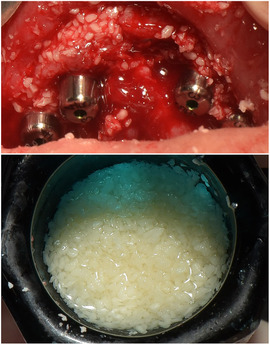
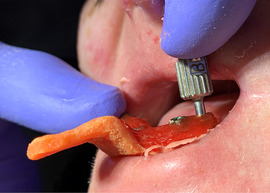
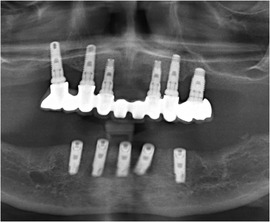
Aims: To provide (a) a complete review of the oral manifestations in those living with each type of inherited EB, (b) the current best practices for managing oral health care of people living with EB, (c) the current best practices on dental implant-based oral rehabilitation for patients with recessive dystrophic EB (RDEB), and (d) the current best practice for managing local anesthesia, principles of sedation, and general anesthesia for children and adults with EB undergoing dental treatment.
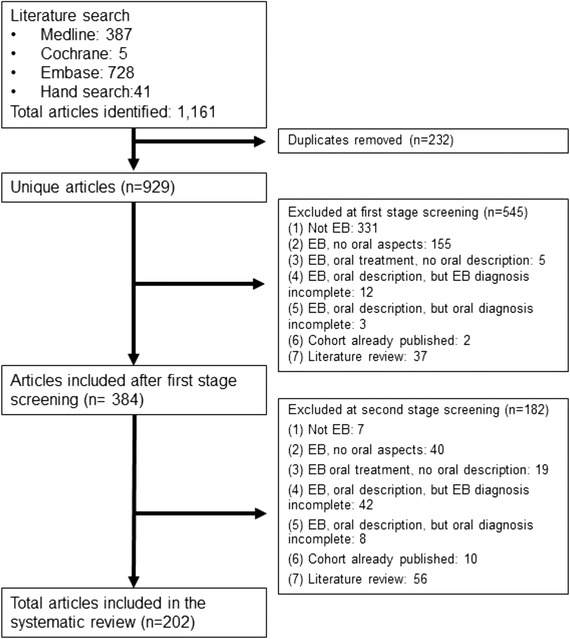
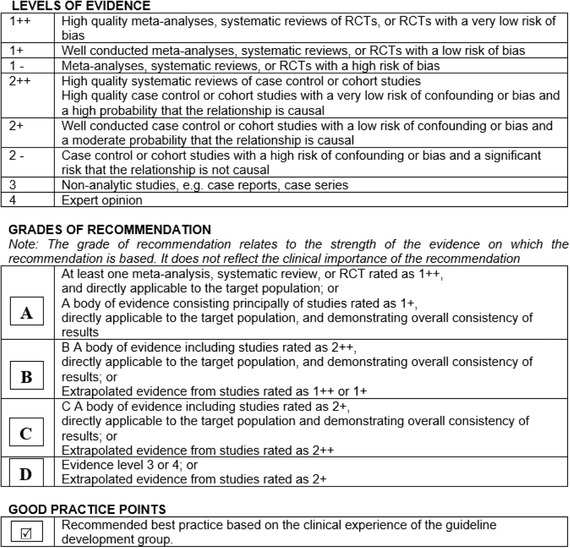
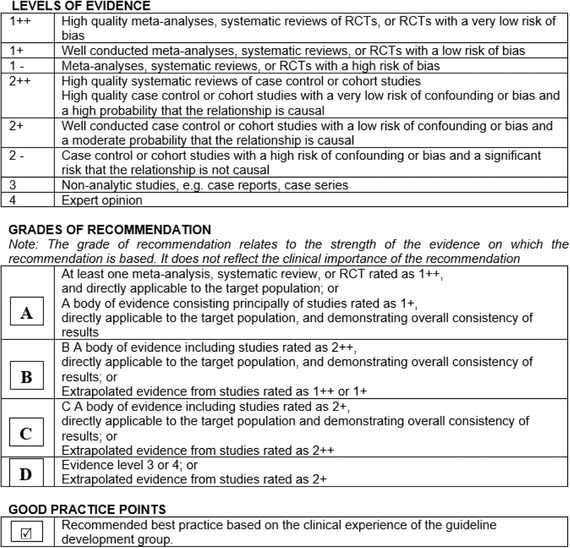
Methods: Systematic literature search, panel discussion including clinical experts and patient representatives from different centers around the world, external review, and guideline piloting.
Results: This article has been divided into five chapters: (i) general information on EB for the oral health care professional, (ii) systematic literature review on the oral manifestations of EB, (iii) oral health care and dental treatment for children and adults living with EB-clinical practice guidelines, (iv) dental implants in patients with RDEB-clinical practice guidelines, and (v) sedation and anesthesia for adults and children with EB undergoing dental treatment-clinical practice guidelines. Each chapter provides recommendations on the management of the different clinical procedures within dental practice, highlighting the importance of patient-clinician partnership, impact on quality of life, and the importance of follow-up appointments. Guidance on the use on nonadhesive wound care products and emollients to reduce friction during patient care is provided.
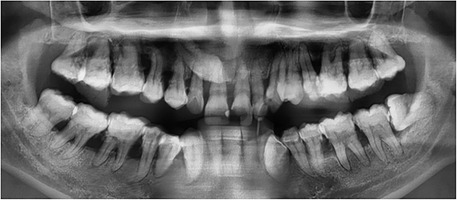
Conclusions: Oral soft and hard tissue manifestations of inherited EB have unique patterns of involvement associated with each subtype of the condition. Understanding each subtype individually will help the professionals plan long-term treatment approaches.
Keywords: clinical practice guideline; dental implants; dental treatment; dystrophic epidermolysis bullosa; epidermolysis bullosa; epidermolysis bullosa simplex; general anesthesia; junctional epidermolysis bullosa; kindler epidermolysis bullosa; oral care; oral rehabilitation; recessive dystrophic epidermolysis bullosa; sedation.
© 2020 The Authors. Special Care in Dentistry published by Special Care Dentistry Association and Wiley Periodicals LLC.
Conflict of interest statement
None of the authors declared conflict of interest. None of the authors has any connection to manufacturers.
Figures















































































References
-
- Krämer SM, Serrano MC, Zillmann G, et al. Oral health care for patients with epidermolysis bullosa ‐ best clinical practice guidelines. Int J Paediatr Dent. 2012;22:1‐35. - PubMed
-
- Pearson RW. Studies on the pathogenesis of epidermolysis bullosa. J Invest Dermatol. 1962;39(6):551‐575. - PubMed
-
- Fine JD, Eady RAJ, Bauer EA, et al. The classification of inherited epidermolysis bullosa (EB): Report of the Third International Consensus Meeting on Diagnosis and Classification of EB. J Am Acad Dermatol. 2008;58(6):931‐950. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
