

Opioid Preconditioning Modulates Repair Responses to Prevent Renal Ischemia-Reperfusion Injury
- PMID: 33202532
- PMCID: PMC7696679
- DOI: 10.3390/ph13110387
Opioid Preconditioning Modulates Repair Responses to Prevent Renal Ischemia-Reperfusion Injury
Abstract
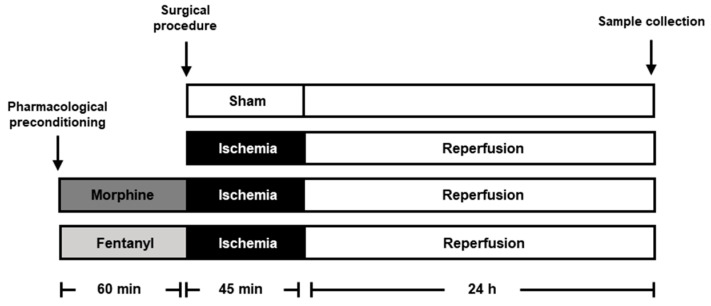
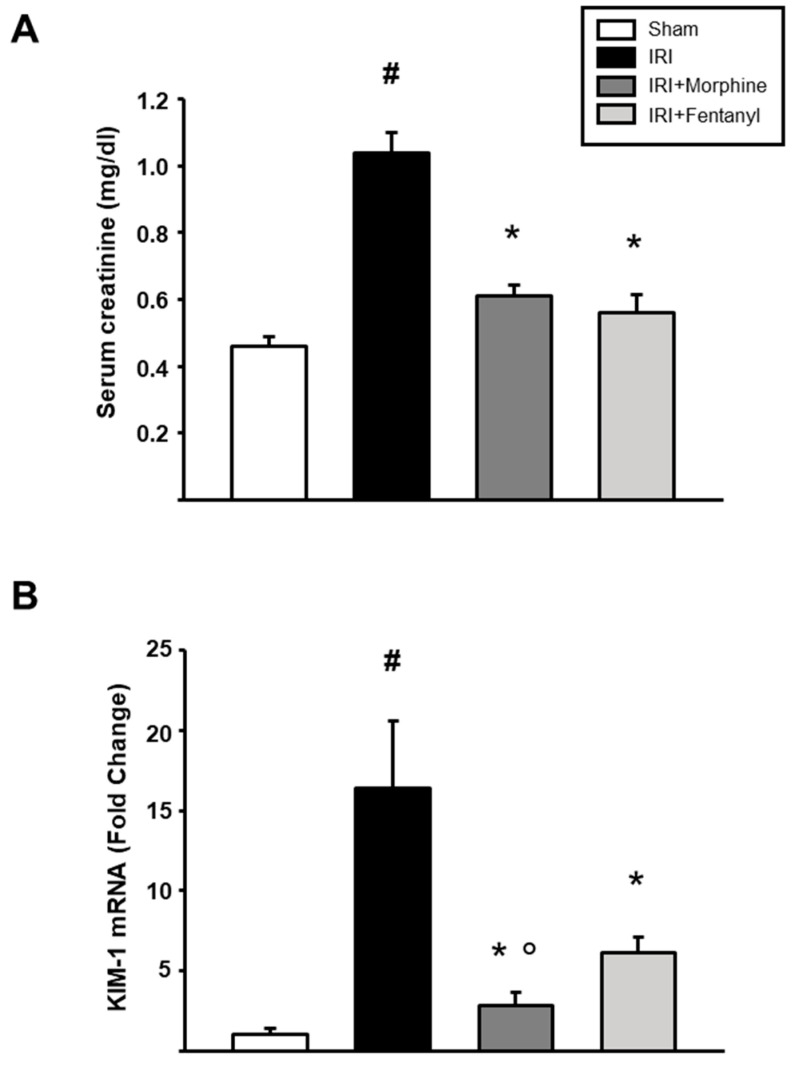
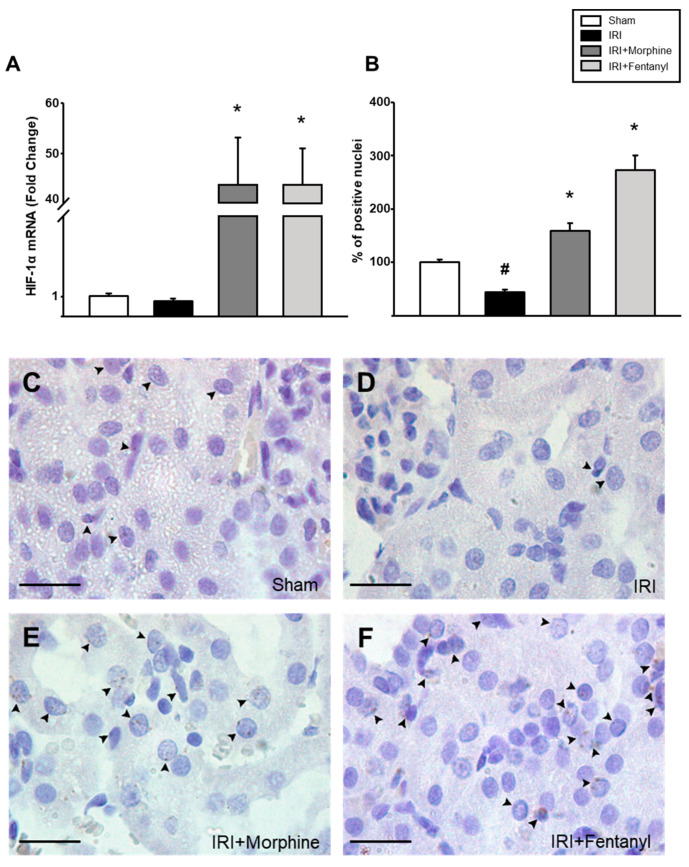
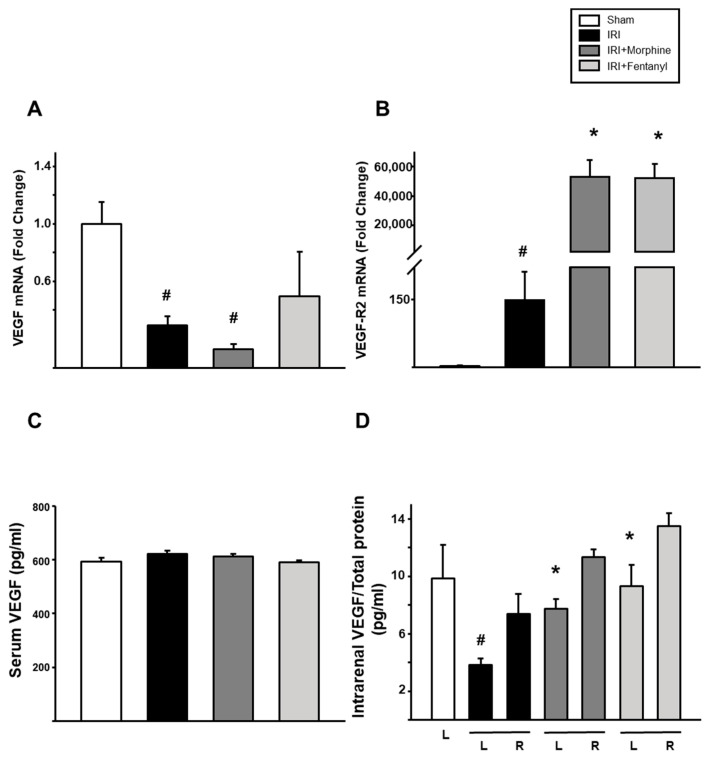
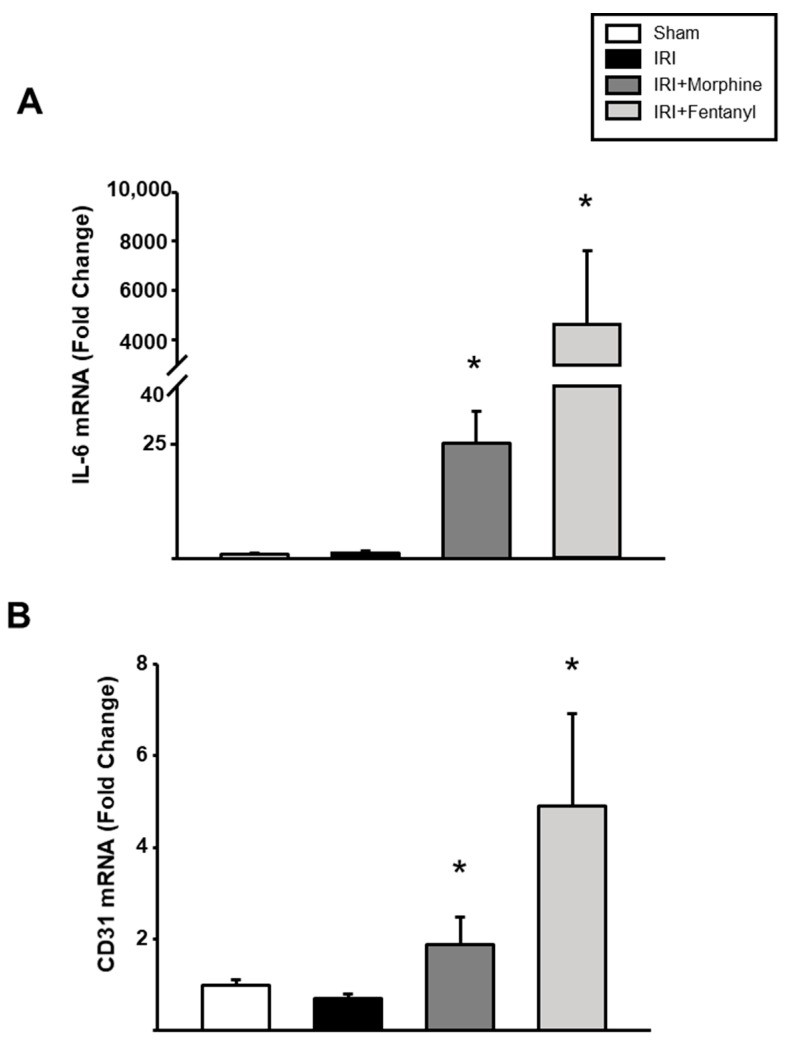
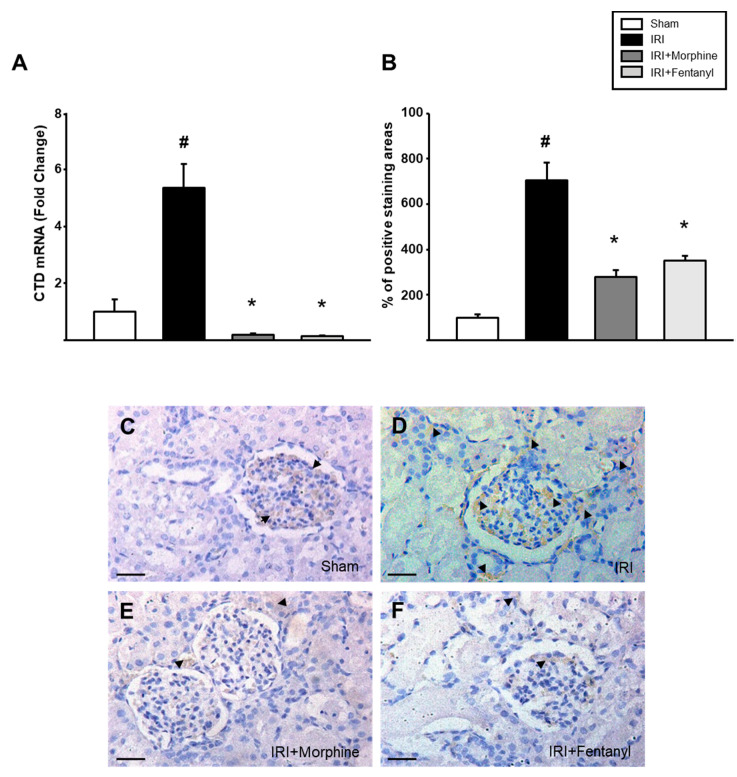
Progression to renal damage by ischemia-reperfusion injury (IRI) is the result of the dysregulation of various tissue damage repair mechanisms. Anesthetic preconditioning with opioids has been shown to be beneficial in myocardial IRI models. Our main objective was to analyze the influence of pharmacological preconditioning with opioids in renal function and expression of molecules involved in tissue repair and angiogenesis. Experimental protocol includes male rats with 45 min ischemia occluding the left renal hilum followed by 24 h of reperfusion with or without 60 min preconditioning with morphine/fentanyl. We analyzed serum creatinine and renal KIM-1 expression. We measured circulating and intrarenal VEGF. Immunohistochemistry for HIF-1 and Cathepsin D (CTD) and real-time PCR for angiogenic genes HIF-1α, VEGF, VEGF Receptor 2 (VEGF-R2), CTD, CD31 and IL-6 were performed. These molecules are considered important effectors of tissue repair responses mediated by the development of new blood vessels. We observed a decrease in acute renal injury mediated by pharmacological preconditioning with opioids. Renal function in opioid preconditioning groups was like in the sham control group. Both anesthetics modulated the expression of HIF-1, VEGF, VEGF-R2 and CD31. Preconditioning negatively regulated CTD. Opioid preconditioning decreased injury through modulation of angiogenic molecule expression. These are factors to consider when establishing strategies in pathophysiological and surgical processes.
Keywords: angiogenesis; fentanyl; morphine; opioids; renal ischemia-reperfusion; wound healing.
Conflict of interest statement
The authors declare no conflict of interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
