

Spontaneous Remission and Concomitant Progression in a Patient with DLBCL
- PMID: 33202678
- PMCID: PMC7697978
- DOI: 10.3390/diagnostics10110950
Spontaneous Remission and Concomitant Progression in a Patient with DLBCL
Abstract
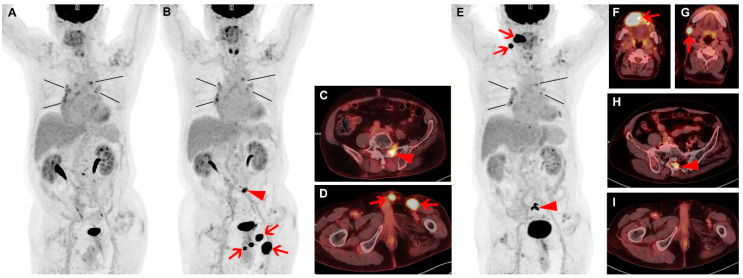
Diffuse large B-cell lymphoma (DLBCL) is the most common type of lymphoma. Although DLBCL can be cured in more than half of all patients, up to 50% of patients become refractory to initial treatment or relapse after complete remission. We present a case of complete spontaneous remission of some tumors and concomitant newly developed tumors observed in a patient with relapsed DLBCL. Spontaneous remission of lymphoma without treatment is a rare phenomenon and can occur at baseline as well as in relapsed DLBCL. However, most patients who initially experience spontaneous remission later develop relapse. Thus, careful follow-up is required, and fluorine-18-fluorodeoxyglucose (18F-FDG) positron emission tomography (PET)/computed tomography (CT) allows monitoring of multiple lesions.
Keywords: FDG; PET/CT; diffuse large B-cell lymphoma; spontaneous remission.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Crump M., Neelapu S.S., Farooq U., Van Den Neste E., Kuruvilla J., Westin J., Link B.K., Hay A., Cerhan J.R., Zhu L., et al. Outcomes in refractory diffuse large B-cell lymphoma: results from the international SCHOLAR-1 study. Blood. 2017;130:1800–1808. doi: 10.1182/blood-2017-03-769620. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
