

Cervical Spine Alignment in the Sagittal Axis: A Review of the Best Validated Measures in Clinical Practice
- PMID: 33203239
- PMCID: PMC8453677
- DOI: 10.1177/2192568220972076
Cervical Spine Alignment in the Sagittal Axis: A Review of the Best Validated Measures in Clinical Practice
Abstract
Study design: Review of the best-validated measures of cervical spine alignment in the sagittal axis.
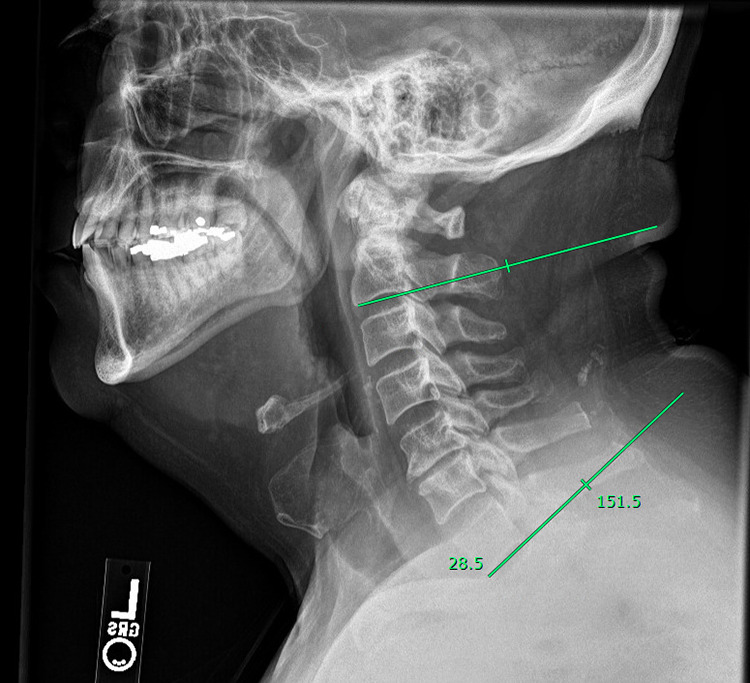
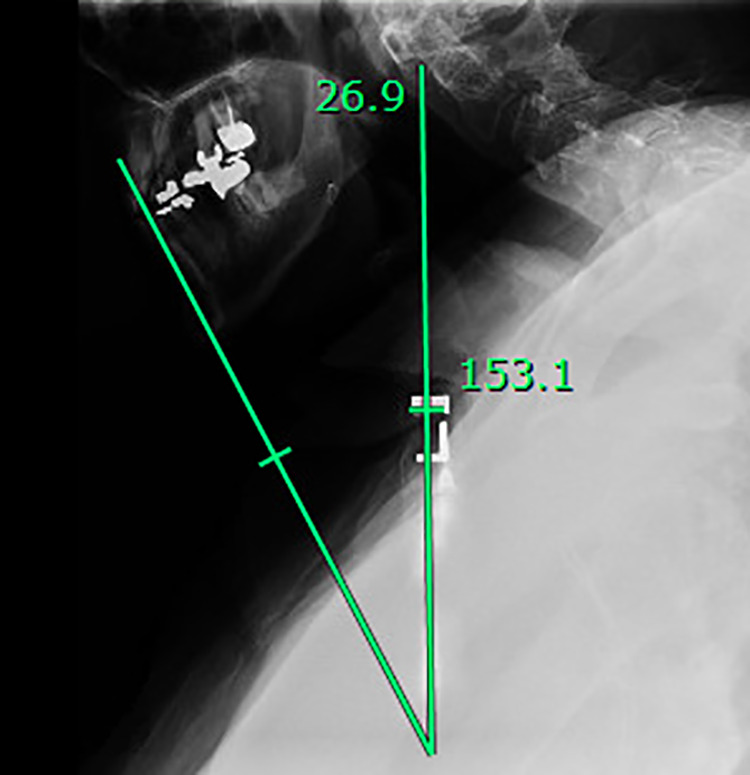
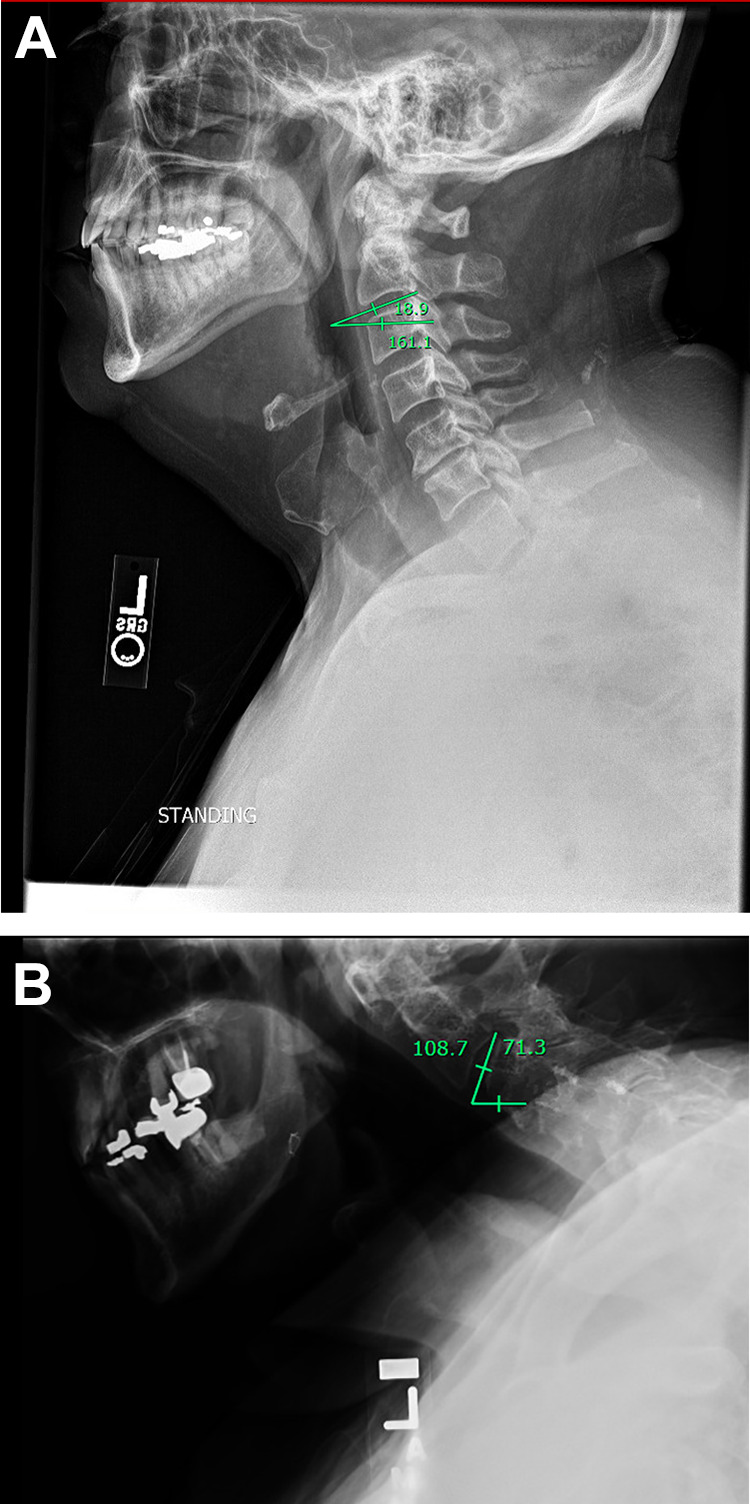
Objective: Describe the C2-C7 Cobb Angle, C2-C7 sagittal vertical axis, chin-brow to vertical angle, T1 slope minus C2-C7 lordosis, C2 slope, and different types of cervical kyphosis.
Methods: Search PubMed for recent technical literature on radiograph-based measurements of the cervical spine.
Results: Despite the continuing use of measures developed many years ago such as the C2-C7 Cobb angle, there are new radiographic parameters being published and utilized in recent years, including the C2 slope. Further research is needed to compare older and newer measures for cross-validation. Utilizing these measures to determine the degree of correction intraoperatively and postoperatively will enable surgeons to optimize patient-level outcomes.
Conclusion: Cervical spinal deformity can be a debilitating condition characterized by cervical spinal misalignment that affects the elderly more commonly than young populations. Many of these validated measures of cervical spinal alignment are useful in clinical settings due to their ease of implementation and correlations with various postoperative and health-related quality of life outcomes.
Keywords: C2 slope; T1 slope; cervical spinal deformity; cobb angle; horizontal gaze; kyphosis; lordosis; sagittal vertical axis.
Conflict of interest statement
Figures


References
-
- Gore DR, Sepic SB, Gardner GM. Roentgenographic findings of the cervical spine in asymptomatic people. Spine (Phila Pa 1976). 1986;11(6):521–524. - PubMed
-
- Harrison DE, Harrison DD, Cailliet R, Troyanovich SJ, Janik TJ, Holland B. Cobb method or Harrison posterior tangent method: which to choose for lateral cervical radiographic analysis. Spine (Phila Pa 1976). 2000;25(16):2072–2078. - PubMed
-
- Tang R, Ye IB, Cheung ZB, Kim JS, Cho SK. Age-related changes in cervical sagittal alignment: a radiographic analysis. Spine (Phila Pa 1976). 2019;44(19):E1144–E1150. - PubMed
-
- Ames CP, Smith JS, Eastlack R, et al. Reliability assessment of a novel cervical spine deformity classification system. J Neurosurg Spine. 2015;23(6):673–683. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
