

A randomized phase II trial evaluating the addition of low dose, short course sunitinib to docetaxel in advanced solid tumours
- PMID: 33203399
- PMCID: PMC7672922
- DOI: 10.1186/s12885-020-07616-4
A randomized phase II trial evaluating the addition of low dose, short course sunitinib to docetaxel in advanced solid tumours
Abstract
Background: We previously reported that low-dose, short-course sunitinib prior to neoadjuvant doxorubicin-cyclophosphamide (AC) normalised tumour vasculature and improved perfusion, but resulted in neutropenia and delayed subsequent cycles in breast cancer patients. This study combined sunitinib with docetaxel, which has an earlier neutrophil nadir than AC.
Methods: Patients with advanced solid cancers were randomized 1:1 to 3-weekly docetaxel 75 mg/m2, with or without sunitinib 12.5 mg daily for 7 days prior to docetaxel, stratified by primary tumour site. Primary endpoints were objective-response (ORR:CR + PR) and clinical-benefit rate (CBR:CR + PR + SD); secondary endpoints were toxicity and progression-free-survival (PFS).
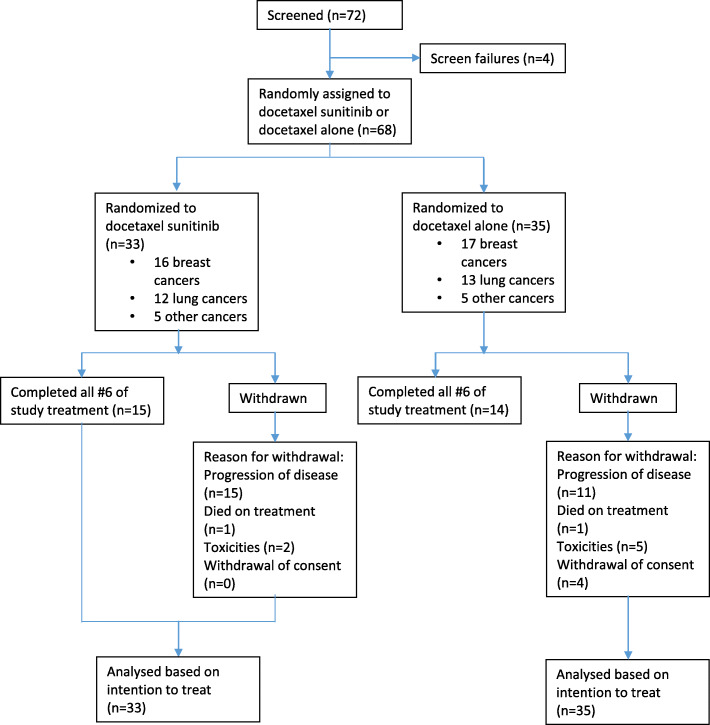
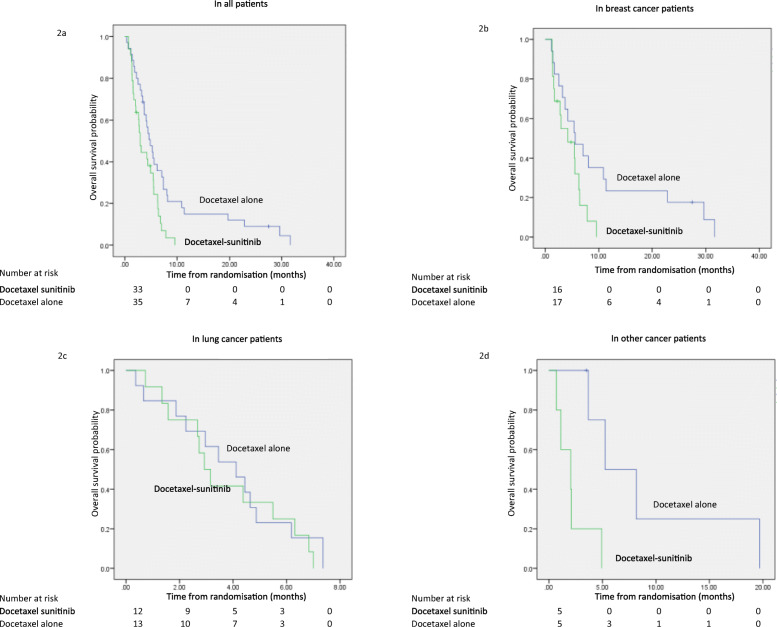
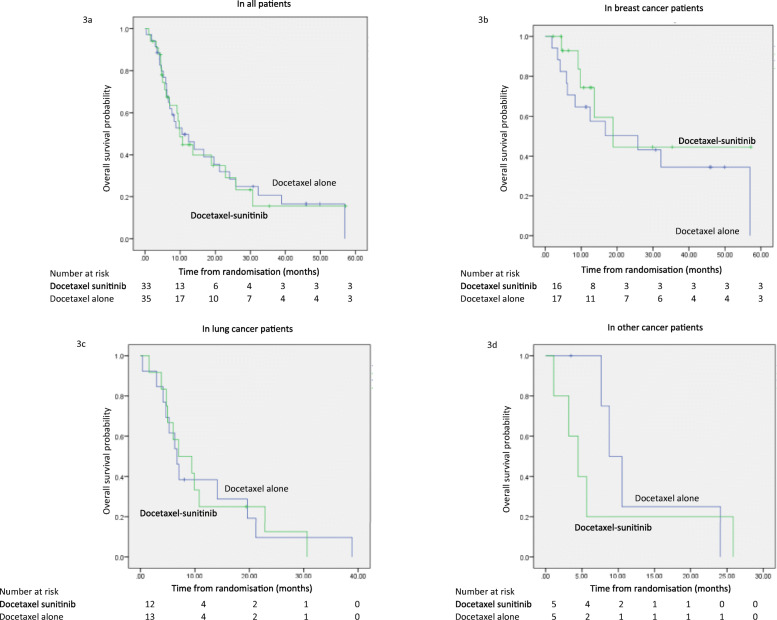
Results: We enrolled 68 patients from 2 study sites; 33 received docetaxel-sunitinib and 35 docetaxel alone, with 33 breast, 25 lung and 10 patients with other cancers. There was no difference in ORR (30.3% vs 28.6%, p = 0.432, odds-ratio [OR] 1.10, 95% CI 0.38-3.18); CBR was lower in the docetaxel-sunitinib arm (48.5% vs 71.4%, p = 0.027 OR 0.37, 95% CI 0.14-1.01). Median PFS was shorter in the docetaxel-sunitinib arm (2.9 vs 4.9 months, hazard-ratio [HR] 2.00, 95% CI 1.15-3.48, p = 0.014) overall, as well as in breast (4.2 vs 5.6 months, p = 0.048) and other cancers (2.0 vs 5.3 months, p = 0.009), but not in lung cancers (2.9 vs 4.1 months, p = 0.597). Median OS was similar in both arms overall (9.9 vs 10.5 months, HR 0.92, 95% CI 0.51-1.67, p = 0.789), and in the breast (18.9 vs 25.8 months, p = 0.354), lung (7.0 vs 6.7 months, p = 0.970) and other cancers (4.5 vs 8.8 months, p = 0.449) subgroups. Grade 3/4 haematological toxicities were lower with docetaxel-sunitinib (18.2% vs 34.3%, p = 0.132), attributed to greater discretionary use of prophylactic G-CSF (90.9% vs 63.0%, p = 0.024). Grade 3/4 non-haematological toxicities were similar (12.1% vs 14.3%, p = 0.792).
Conclusions: The addition of sunitinib to docetaxel was well-tolerated but did not improve outcomes. The possible negative impact in metastatic breast cancer patients is contrary to results of adding sunitinib to neoadjuvant AC. These negative results suggest that the intermittent administration of sunitinib in the current dose and schedule with docetaxel in advanced solid tumours, particularly breast cancers, is not beneficial.
Trial registration: The study was registered ( NCT01803503 ) prospectively on clinicaltrials.gov on 4th March 2013.
Keywords: Advanced solid tumours; Anti-angiogenic; Docetaxel; Short-course sunitinib; Tumour vasculature.
Conflict of interest statement
RAS: Honoraria: Astra Zeneca, BMS, Boehringer Ingelheim, Eli-Lilly, Merck, Novartis, Pfizer, Roche and Taiho; Research grant: Astra-Zeneca.
RS: Advisory board: BMS, Merck, Eisai, Bayer, Taiho; honoraria for talks: MSD, Eli Lilly, BMS, Roche, Taiho; Travel funding: Roche, Astra Zeneca, Taiho, Eisai; Research funding: Paxman Coolers, MSD.
These are outside the submitted work.
SGWO: Honoraria: Pfizer, Astra Zeneca, Novartis, Eli Lily.
BCT: Honoraria for workshops: Boehringer Ingelheim; Royalty: Wiley-Blackwell.
SCL: Advisory board: Roche, MSD, Astra Zeneca, Pfizer, Novartis, Eli Lilly, ACT Genomics, Eisai; honoraria for talks: Astra Zeneca, Pfizer, Novartis, ACT Genomics, Eisai; Research Funding: Taiho, Eisai, Pfizer, ACT Genomics, ASLAN Pharmaceuticals Ltd.; Travel funding for conferences: Amgen, Pfizer.
The other authors declare that they have no competing interests.
Figures
References
-
- Carrato A, Swieboda-Sadlej A, Staszewska-Skurczynska M, Lim R, Roman L, Shparyk Y, et al. Fluorouracil, leucovorin, and irinotecan plus either sunitinib or placebo in metastatic colorectal cancer: a randomized, phase III trial. J Clin Oncol. 2013;31(10):1341–1347. doi: 10.1200/JCO.2012.45.1930. - DOI - PubMed
-
- Bergh J, Bondarenko IM, Lichinitser MR, Liljegren A, Greil R, Voytko NL, et al. First-line treatment of advanced breast cancer with sunitinib in combination with docetaxel versus docetaxel alone: results of a prospective, randomized phase III study. J Clin Oncol. 2012;30(9):921–929. doi: 10.1200/JCO.2011.35.7376. - DOI - PubMed
-
- Paz-Ares LG, Biesma B, Heigener D, von Pawel J, Eisen T, Bennouna J, et al. Phase III, randomized, double-blind, placebo-controlled trial of gemcitabine/cisplatin alone or with sorafenib for the first-line treatment of advanced, nonsquamous non-small-cell lung cancer. J Clin Oncol. 2012;30(25):3084–3092. doi: 10.1200/JCO.2011.39.7646. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
