

Development of pre-syrinx state and syringomyelia following a minor injury: a case report
- PMID: 33203466
- PMCID: PMC7672986
- DOI: 10.1186/s13256-020-02568-6
Development of pre-syrinx state and syringomyelia following a minor injury: a case report
Abstract
Background: A generally accepted rule is that posttraumatic syringomyelia (PTS) results from spinal cord injury (SCI).
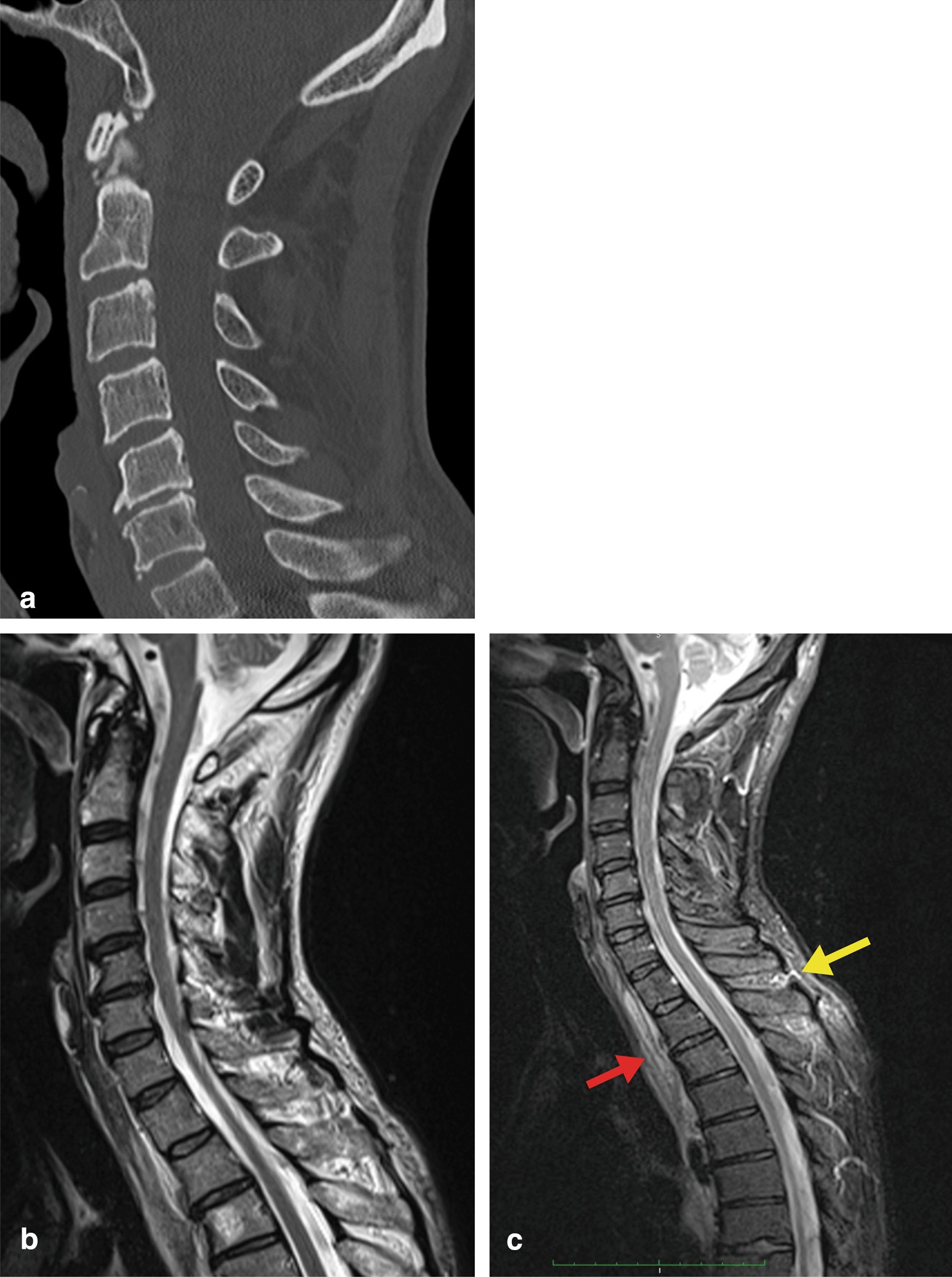
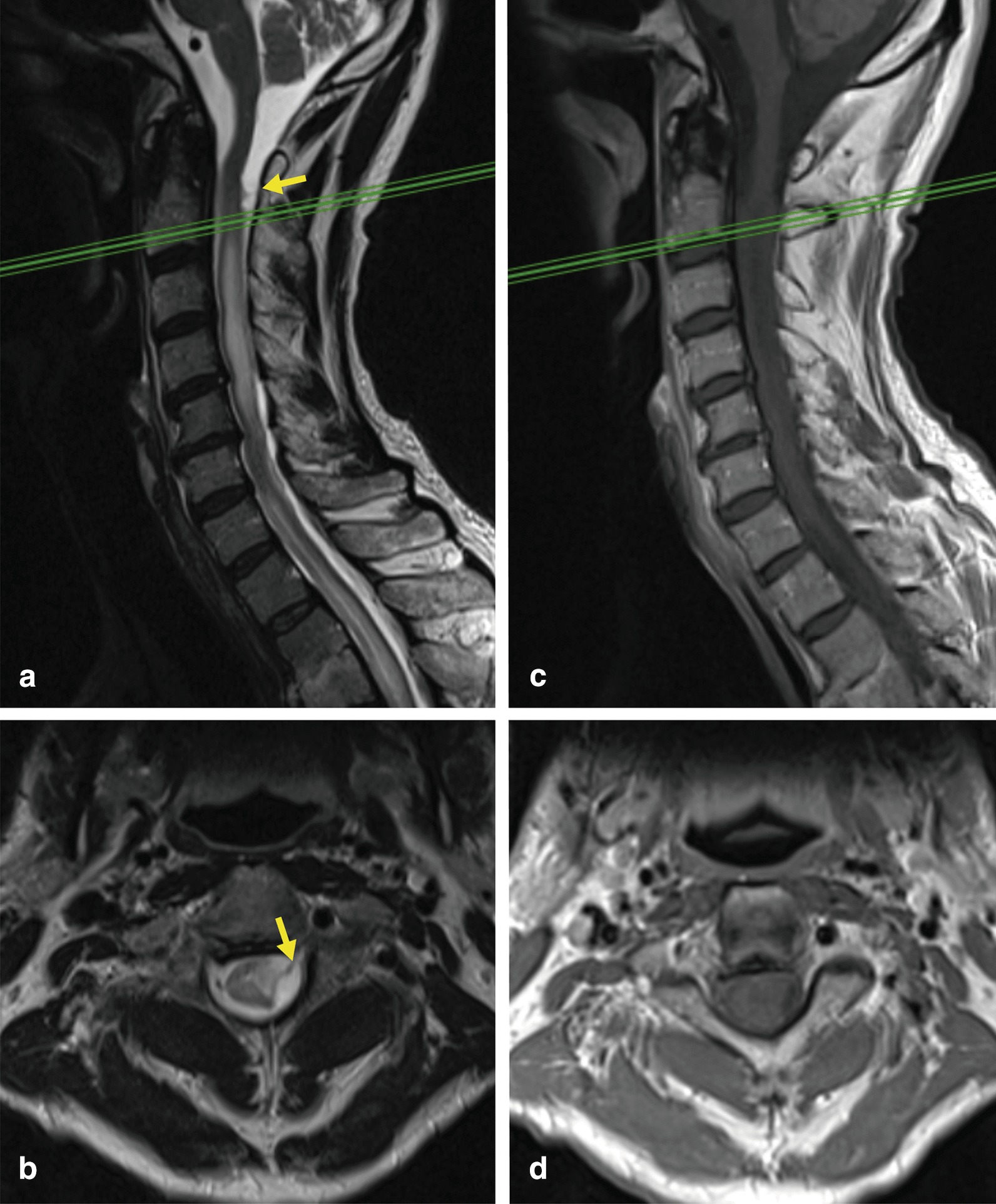
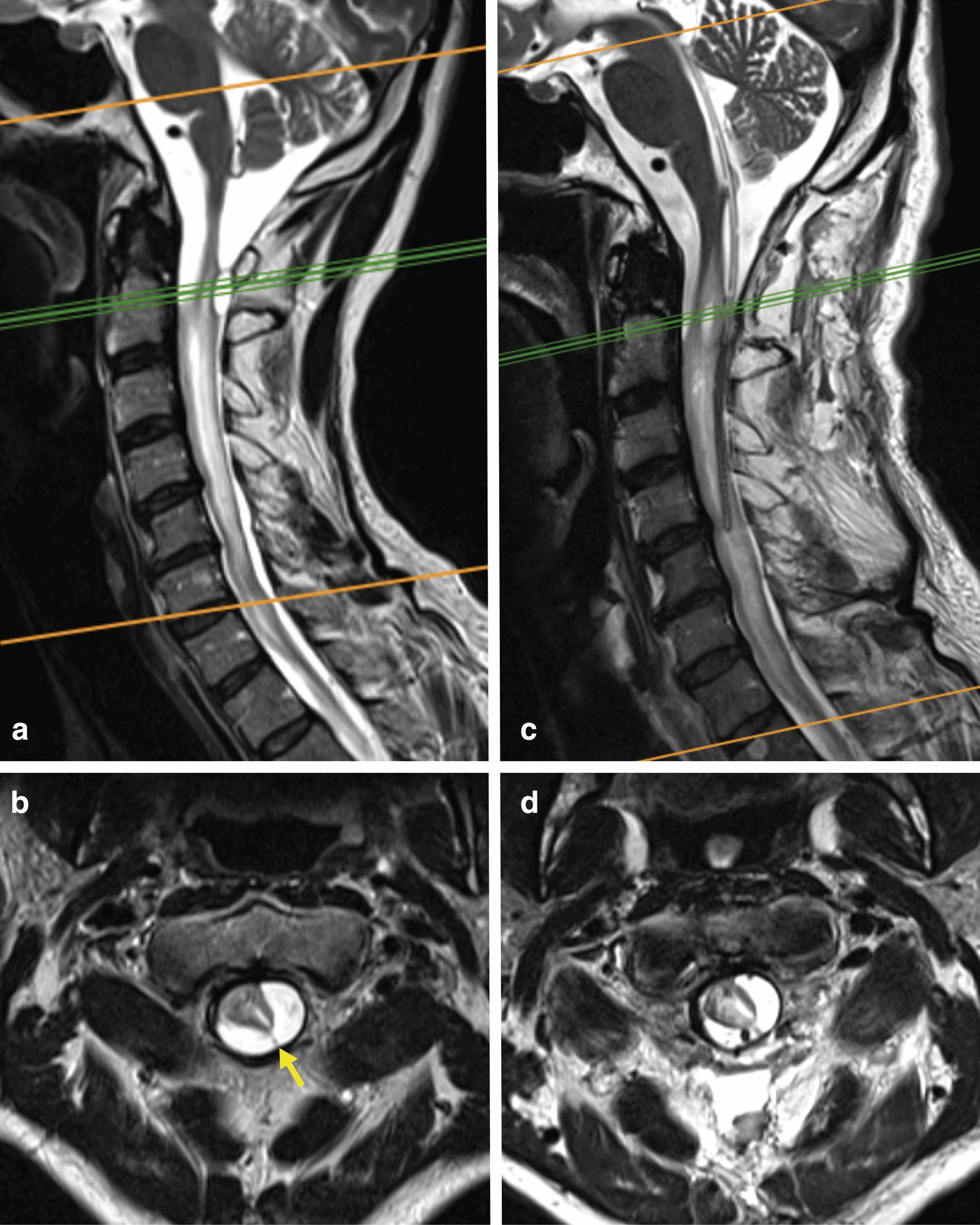
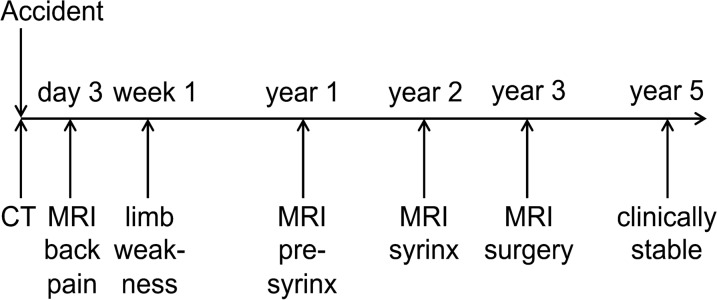
Case presentation: Here, we report the development of syringomyelia without SCI in a 54-year-old Caucasian man following a mild motor vehicle accident. The computed tomography on admission excluded an injury of the spine. Because of neck and back pain, magnetic resonance imaging was performed on day 3 post-injury and demonstrated minimal changes from a ligamentous strain at the cervicothoracic transition. Any traumatic affection of the bone, vertebral discs, intraspinal compartment, or spinal cord were excluded. Some limb weakness and neurogenic bladder dysfunction started manifesting within the following weeks. Repeated MRIs following the accident demonstrated arachnoid adhesions at the C1-2 level and spinal cord edema equivalent to a pre-syrinx state at 12 months and syrinx formation at 24 months. Because of further deterioration, decompression was performed at 36 months.
Conclusions: We conclude that even after a minor trauma PTS can occur and that medullary edema (pre-syrinx state) may precede syrinx formation.
Keywords: Pre-syrinx; Spinal cord injury; Syringomyelia; Trauma; Treatment.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
The role of acute decompression and restoration of spinal alignment in the prevention of post-traumatic syringomyelia: case report and review of recent literature.Spine (Phila Pa 1976). 2001 Sep 1;26(17):E399-402. doi: 10.1097/00007632-200109010-00028. Spine (Phila Pa 1976). 2001. PMID: 11568717
-
The characteristics of posttraumatic syringomyelia.Spinal Cord. 2016 Jun;54(6):463-6. doi: 10.1038/sc.2015.218. Epub 2015 Dec 1. Spinal Cord. 2016. PMID: 26620880
-
C-5 palsy after cerebrospinal fluid diversion in posttraumatic syringomyelia: case report.J Neurosurg Spine. 2015 Apr;22(4):394-8. doi: 10.3171/2014.10.SPINE14315. Epub 2015 Feb 6. J Neurosurg Spine. 2015. PMID: 25658467
-
Treatment of posttraumatic syringomyelia: evidence from a systematic review.Acta Neurochir (Wien). 2020 Oct;162(10):2541-2556. doi: 10.1007/s00701-020-04529-w. Epub 2020 Aug 20. Acta Neurochir (Wien). 2020. PMID: 32820376 Free PMC article.
-
Radiographic assessment of surgical treatment of post-traumatic syringomyelia.J Spinal Cord Med. 2021 Nov;44(6):861-869. doi: 10.1080/10790268.2020.1743086. Epub 2020 Mar 30. J Spinal Cord Med. 2021. PMID: 32223591 Free PMC article. Review.
Cited by
-
Spinal Adhesive Arachnoidopathy, the Disorder More Than Simply Adhesive Arachnoiditis: A Comprehensive Systematic Review of 510 Cases.CNS Neurosci Ther. 2024 Oct;30(10):e70084. doi: 10.1111/cns.70084. CNS Neurosci Ther. 2024. PMID: 39435986 Free PMC article.
-
Delta Cord as a Radiological Localization Sign of Postoperative Adhesive Arachnoiditis: A Case Report and Literature Review.Diagnostics (Basel). 2023 Sep 14;13(18):2942. doi: 10.3390/diagnostics13182942. Diagnostics (Basel). 2023. PMID: 37761311 Free PMC article.
-
Spinal cord untethering and midline myelotomy for delayed, symptomatic post-traumatic syringomyelia due to retained ballistic fragments: case report.Spinal Cord Ser Cases. 2022 Jul 12;8(1):66. doi: 10.1038/s41394-022-00533-7. Spinal Cord Ser Cases. 2022. PMID: 35831274 Free PMC article.
References
-
- Milhorat TH, Johnson RW, Milhorat RH, Capocelli AL, Jr, Pevsner PH. Clinicopathological correlations in syringomyelia using axial magnetic resonance imaging. Neurosurgery. 1995;37(2):206–213. - PubMed
-
- Fairholm DJ, Turnbull IM. Microangiographic study of experimental spinal cord injuries. J Neurosurg. 1971;35(3):277–286. - PubMed
-
- Cho KH, Iwasaki Y, Imamura H, Hida K, Abe H. Experimental model of posttraumatic syringomyelia: the role of adhesive arachnoiditis in syrinx formation. J Neurosurg. 1994;80(1):133–139. - PubMed
-
- Abel R, Gerner HJ, Smit C, Meiners T. Residual deformity of the spinal canal in patients with traumatic paraplegia and secondary changes of the spinal cord. Spinal Cord. 1999;37(1):14–19. - PubMed
-
- Perrouin-Verbe B, Robert R, Lefort M, Agakhani N, Tadie M, Mathe JF. Post-traumatic syringomyelia. Neurochirurgie. 1999;45(Suppl 1):58–66. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
