

Estimated impact of the COVID-19 pandemic on cancer services and excess 1-year mortality in people with cancer and multimorbidity: near real-time data on cancer care, cancer deaths and a population-based cohort study
- PMID: 33203640
- PMCID: PMC7674020
- DOI: 10.1136/bmjopen-2020-043828
Estimated impact of the COVID-19 pandemic on cancer services and excess 1-year mortality in people with cancer and multimorbidity: near real-time data on cancer care, cancer deaths and a population-based cohort study
Abstract
Objectives: To estimate the impact of the COVID-19 pandemic on cancer care services and overall (direct and indirect) excess deaths in people with cancer.
Methods: We employed near real-time weekly data on cancer care to determine the adverse effect of the pandemic on cancer services. We also used these data, together with national death registrations until June 2020 to model deaths, in excess of background (pre-COVID-19) mortality, in people with cancer. Background mortality risks for 24 cancers with and without COVID-19-relevant comorbidities were obtained from population-based primary care cohort (Clinical Practice Research Datalink) on 3 862 012 adults in England.
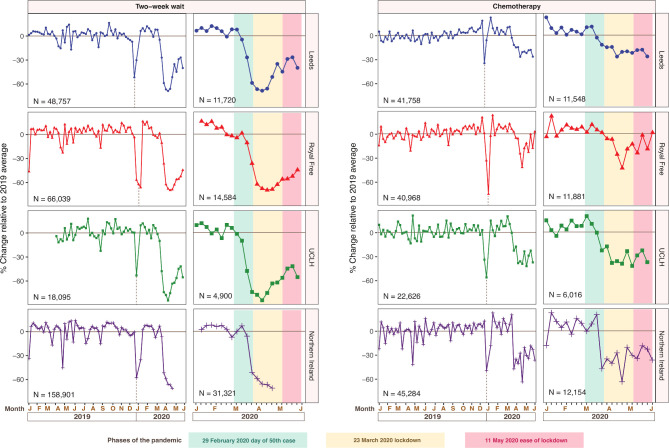
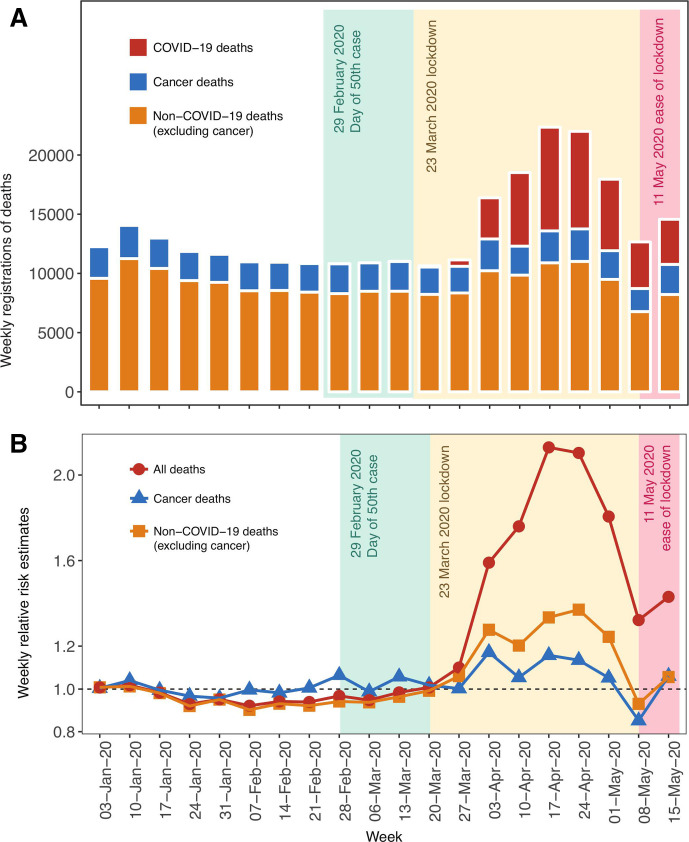
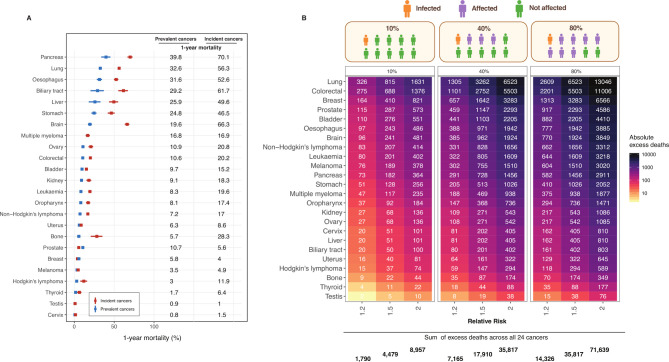
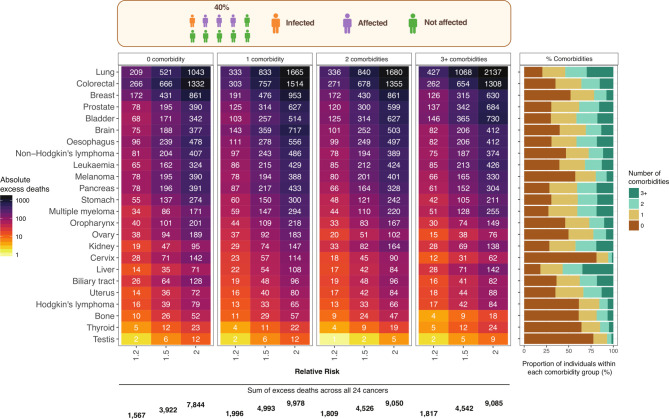
Results: Declines in urgent referrals (median=-70.4%) and chemotherapy attendances (median=-41.5%) to a nadir (lowest point) in the pandemic were observed. By 31 May, these declines have only partially recovered; urgent referrals (median=-44.5%) and chemotherapy attendances (median=-31.2%). There were short-term excess death registrations for cancer (without COVID-19), with peak relative risk (RR) of 1.17 at week ending on 3 April. The peak RR for all-cause deaths was 2.1 from week ending on 17 April. Based on these findings and recent literature, we modelled 40% and 80% of cancer patients being affected by the pandemic in the long-term. At 40% affected, we estimated 1-year total (direct and indirect) excess deaths in people with cancer as between 7165 and 17 910, using RRs of 1.2 and 1.5, respectively, where 78% of excess deaths occured in patients with ≥1 comorbidity.
Conclusions: Dramatic reductions were detected in the demand for, and supply of, cancer services which have not fully recovered with lockdown easing. These may contribute, over a 1-year time horizon, to substantial excess mortality among people with cancer and multimorbidity. It is urgent to understand how the recovery of general practitioner, oncology and other hospital services might best mitigate these long-term excess mortality risks.
Keywords: COVID-19; health informatics; oncology.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: ML has received honoraria from Pfizer, EMD Serono and Roche for presentations unrelated to this research, and an unrestricted educational grant from Pfizer for research unrelated to the research presented in this paper. AB has received research funding from AstraZeneca. MF has received research funding from AstraZeneca, Boehringer Ingelheim, Merck and MSD and honoraria from Achilles, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Meyers Squibb, Celgene, Guardant Health, Merck, MSD, Nanobiotix, Novartis, Pharmamar, Roche and Takeda for advisory roles or presentations unrelated to this research. GF receives funding from companies that manufacture drugs for hepatitis C virus (AbbVie, Gilead, MSD) and is a consultant for GSK, Arbutus and Shionogi in areas unrelated to this research.
Figures
References
-
- Williamson E, Walker AJ, Bhaskaran KJ, et al. OpenSAFELY: factors associated with COVID-19-related Hospital death in the linked electronic health records of 17 million adult NHS patients. MedRxiv 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous