

Entinostat plus Pembrolizumab in Patients with Metastatic NSCLC Previously Treated with Anti-PD-(L)1 Therapy
- PMID: 33203644
- PMCID: PMC7887114
- DOI: 10.1158/1078-0432.CCR-20-3305
Entinostat plus Pembrolizumab in Patients with Metastatic NSCLC Previously Treated with Anti-PD-(L)1 Therapy
Abstract
Purpose: New therapies are needed to treat immune checkpoint inhibitor-resistant non-small cell lung cancer (NSCLC) and identify biomarkers to personalize treatment. Epigenetic therapies, including histone deacetylase inhibitors, may synergize with programmed cell death-1 (PD-1) blockade to overcome resistance. We report outcomes in patients with anti-programmed cell death ligand-1 [PD-(L)1]-resistant/refractory NSCLC treated with pembrolizumab plus entinostat in ENCORE 601.
Patients and methods: The expansion cohort of ENCORE 601 included patients with NSCLC who previously experienced disease progression with immune checkpoint inhibitors. The primary endpoint for the phase II expansion cohort is overall response rate (ORR); safety, tolerability, and exploratory endpoints are described.
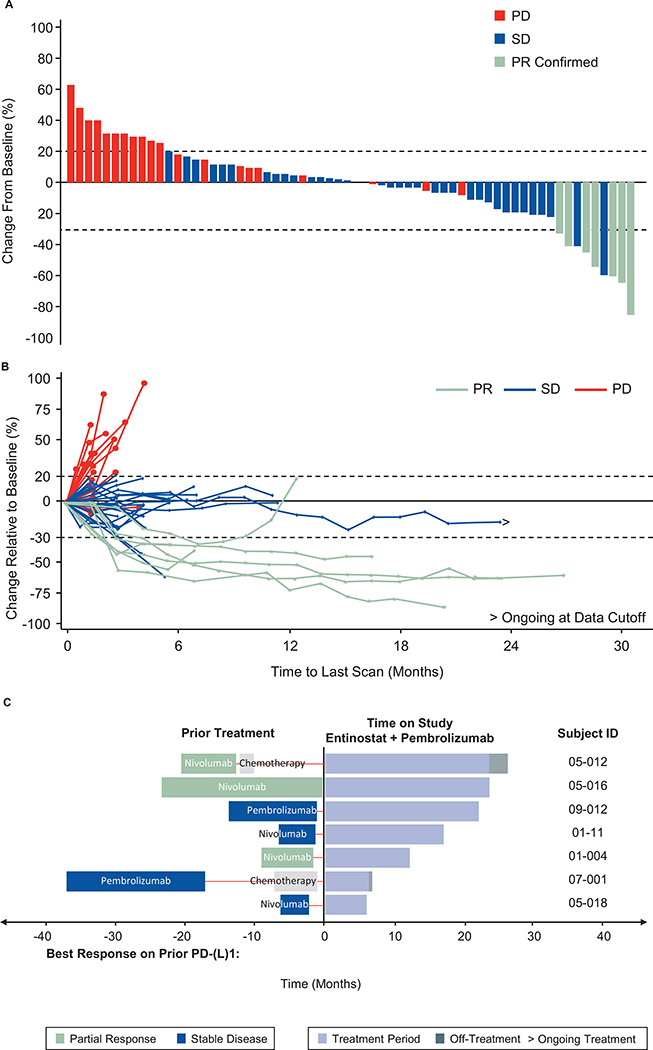
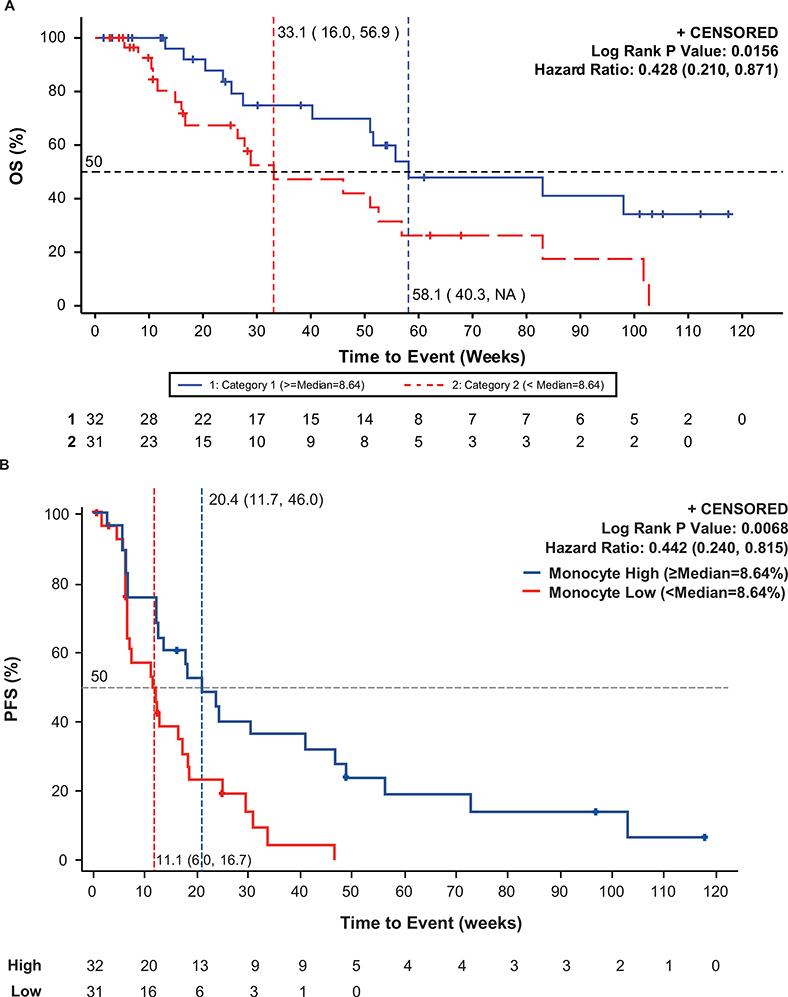
Results: Of 76 treated patients, 71 were evaluable for efficacy. immune-regulated RECIST-assessed ORR was 9.2% [95% confidence interval (CI): 3.8-18.1], which did not meet the prespecified threshold for positivity. Median duration of response was 10.1 months (95% CI: 3.9-not estimable), progression-free survival (PFS) at 6 months was 22%, median PFS was 2.8 months (95% CI: 1.5-4.1), and median overall survival was 11.7 months (95% CI: 7.6-13.4). Benefit was enriched among patients with high levels of circulating classical monocytes at baseline. Baseline tumor PD-L1 expression and IFNγ gene expression were not associated with benefit. Treatment-related grade ≥3 adverse events occurred in 41% of patients.
Conclusions: In anti-PD-(L)1-experienced patients with NSCLC, entinostat plus pembrolizumab did not achieve the primary response rate endpoint but provided a clinically meaningful benefit, with objective response in 9% of patients. No new toxicities, including immune-related adverse events, were seen for either drug. Future studies will continue to evaluate the association of monocyte levels and response.
Trial registration: ClinicalTrials.gov NCT02437136.
©2020 American Association for Cancer Research.
Figures
References
-
- Garon EB, Rizvi NA, Hui R, Leighl N, Balmanoukian AS, Eder JP, et al. Pembrolizumab for the treatment of non–small-cell lung cancer. N Engl J Med. 2015;21372:2018–28. - PubMed
-
- Herbst RS, Baas P, Kim DW, Felip E, Pérez-Gracia JL, Han JY, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet. 2016;387:1540–50. - PubMed
-
- Gandhi L, Rodríguez-Abreu D, Gadgeel S, Esteban E, Felip E, De Angelis F, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018;378:2078–92. - PubMed
-
- Duma N, Santana-Davila R, Molina JR. Non–Small Cell Lung Cancer: Epidemiology, screening, diagnosis, and treatment Mayo Clin Proc. Mayo Foundation for Medical Education and Research; 2019;94:1623–40. - PubMed
-
- FDA. FDA expands pembrolizumab indication for first-line treatment of NSCLC (TPS ≥1%) [Internet]. 2019. [cited 2020 Aug 5]. Available from: https://www.fda.gov/drugs/fda-expands-pembrolizumab-indication-first-lin...
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
