

Completion rate and impact on physician-patient relationship of video consultations in medical oncology: a randomised controlled open-label trial
- PMID: 33203685
- PMCID: PMC7674103
- DOI: 10.1136/esmoopen-2020-000912
Completion rate and impact on physician-patient relationship of video consultations in medical oncology: a randomised controlled open-label trial
Abstract
Background: Mobile phone video call applications generally did not undergo testing in randomised controlled clinical trials prior to their implementation in patient care regarding the rate of successful patient visits and impact on the physician-patient relationship.
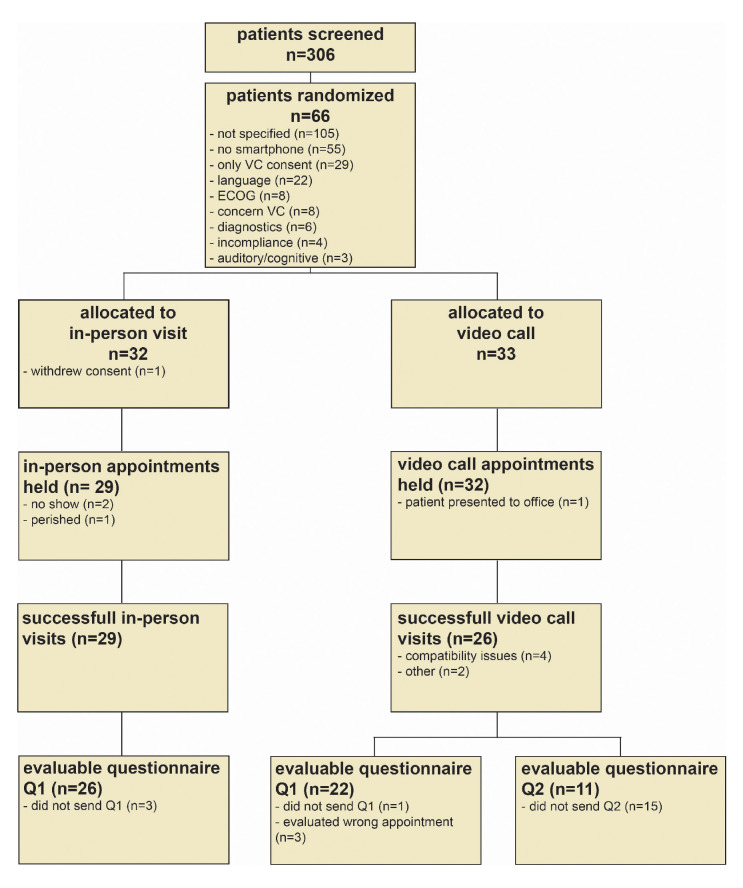
Methods: The National Center for Tumour Diseases (NCT) MOBILE trial was a monocentric open-label randomised controlled clinical trial of patients with solid tumours undergoing systemic cancer therapy with need of a follow-up visit with their consulting physician at outpatient clinics. 66 patients were 1:1 randomised to receive either a standard in-person follow-up visit at outpatient clinics or a video call via a mobile phone application. The primary outcome was feasibility defined as the proportion of patients successfully completing the first follow-up visit. Secondary outcomes included success rate of further video calls, time spent by patient and physician, patient satisfaction and quality of physician-patient relationship.
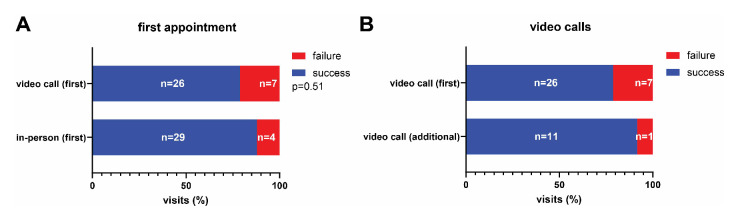
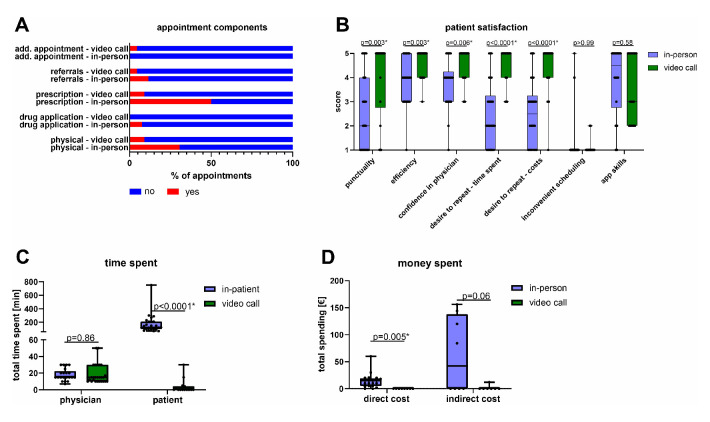
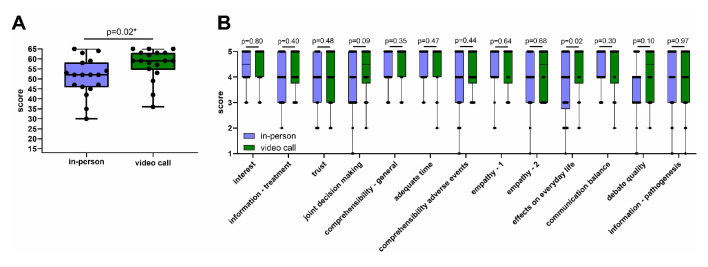
Findings: Success rate of the first follow-up visit in the intention-to-treat cohort was 87.9% (29 of 33) for in-person visits and 78.8% (26 of 33) for video calls (relative risk: RR 0.90, 95% CI 0.70 to 1.13, p=0.51). The most common reasons for failure were software incompatibility in the video call and no-show in the in-person visit arm. The success rate for further video visits was 91.7% (11 of 12). Standardised patient questionnaires showed significantly decreased total time spent and less direct costs for patients (Δmean -170.8 min, 95% CI -246 min to -95.5 min), p<0.0001; Δmean -€14.37, 95% CI -€23.9 to -€4.8, p<0.005) and comparable time spent for physicians in the video call arm (Δmean 0.5 min, 95% CI -5.4 min to 6.4 min, p=0.86). Physician-patient relationship quality mean scores assessed by a validated standardised questionnaire were higher in the video call arm (1.13-fold, p=0.02).
Interpretation: Follow-up visits with the tested mobile phone video call application were feasible but software compatibility should be critically evaluated.
Trial registration number: DRKS00015788.
Keywords: digital health; physician-patient relationship; shared decision-making; smartphone; telemedicine.
© Author (s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. Published by BMJ on behalf of the European Society for Medical Oncology.
Conflict of interest statement
Competing interests: LM is an employee of Minxli, München, Germany.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
