

Urinary Soluble CD163 and Disease Activity in Biopsy-Proven ANCA-Associated Glomerulonephritis
- PMID: 33203735
- PMCID: PMC7769013
- DOI: 10.2215/CJN.07210520
Urinary Soluble CD163 and Disease Activity in Biopsy-Proven ANCA-Associated Glomerulonephritis
Abstract
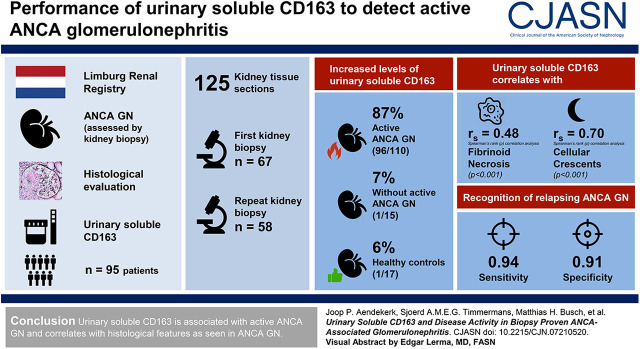
Background and objectives: ANCA-associated GN is a common cause of rapidly progressive GN, with high relapse rates. The early recognition of an ANCA-associated GN relapse is of importance to prevent loss of kidney function. Urinary soluble CD163 has been identified as a promising marker of active ANCA-associated GN. Previous studies, however, are limited by the lack of histologic data.
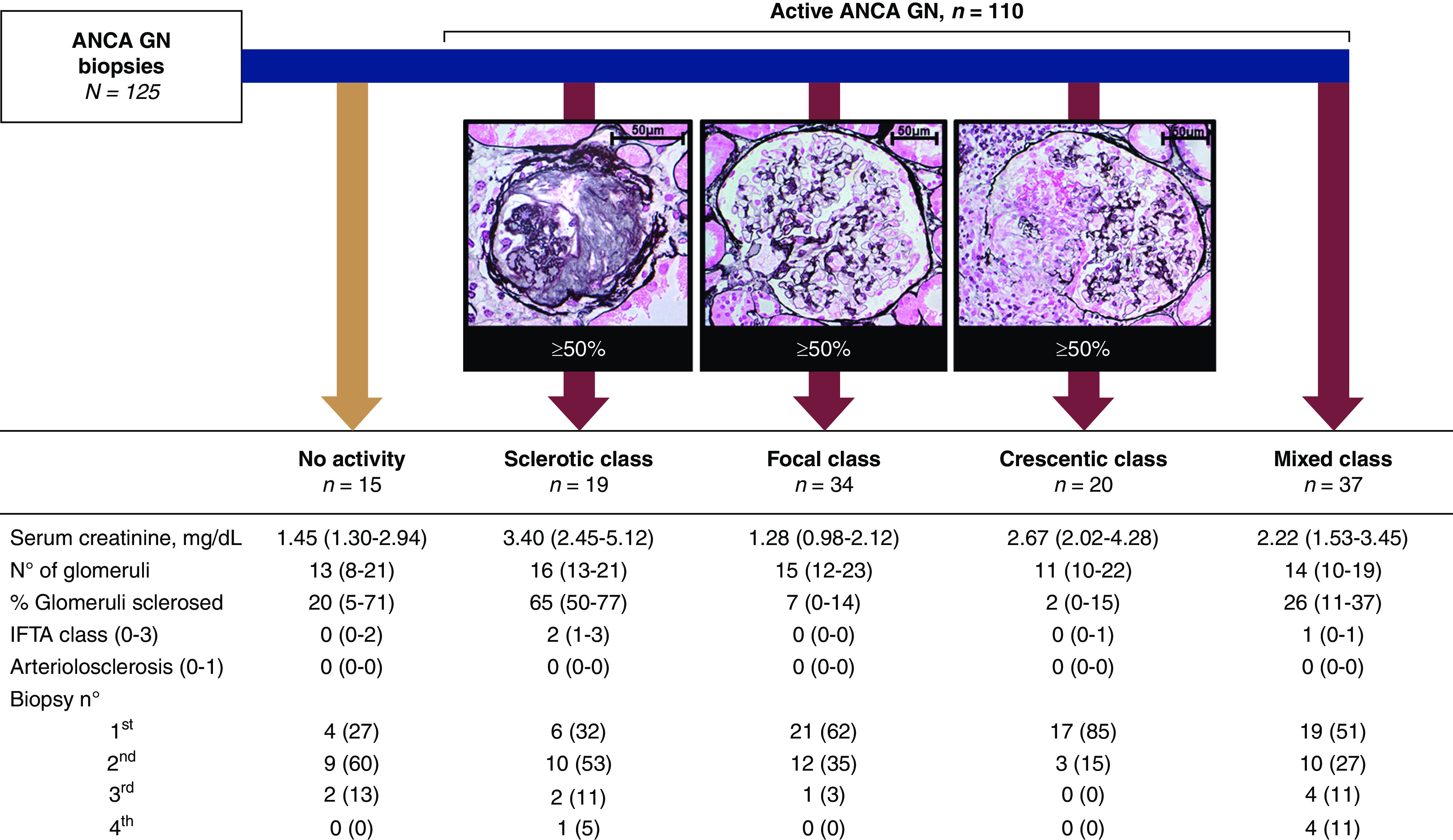
Design, setting, participants, & measurements: We analyzed urinary soluble CD163 in 95 patients with ANCA-associated vasculitis who underwent a kidney biopsy. In total, 125 kidney tissue sections (first kidney biopsy, n=67; repeated biopsy, n=58) with concurrent 24-hour urine samples were studied. Correlation analyses comparing urinary soluble CD163 levels and morphologic features of ANCA-associated GN were performed using Spearman rank correlation analysis. The diagnostic performance of biomarkers to detect relapsing ANCA-associated GN was evaluated using receiver operating characteristics curve analysis.
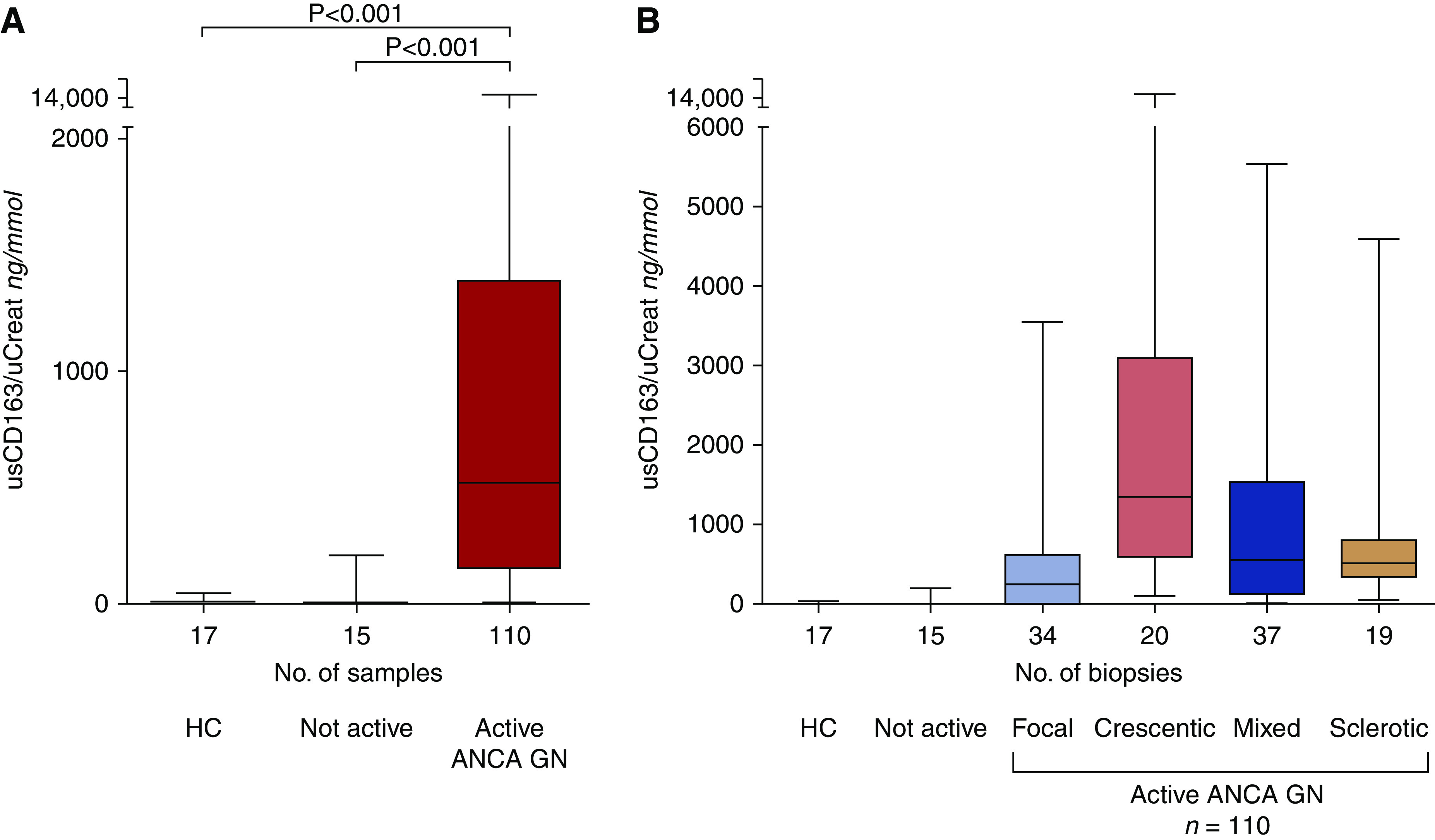
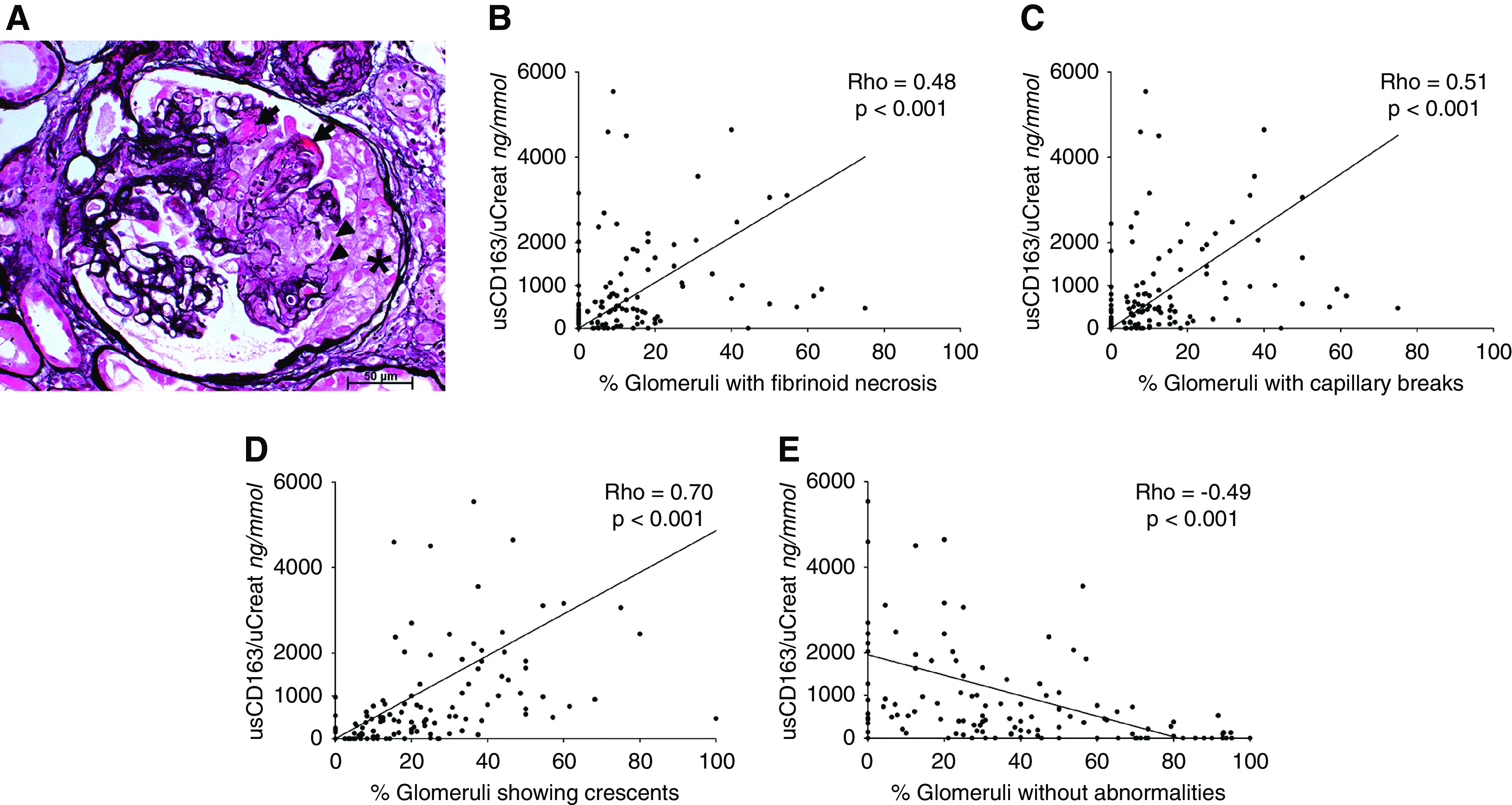
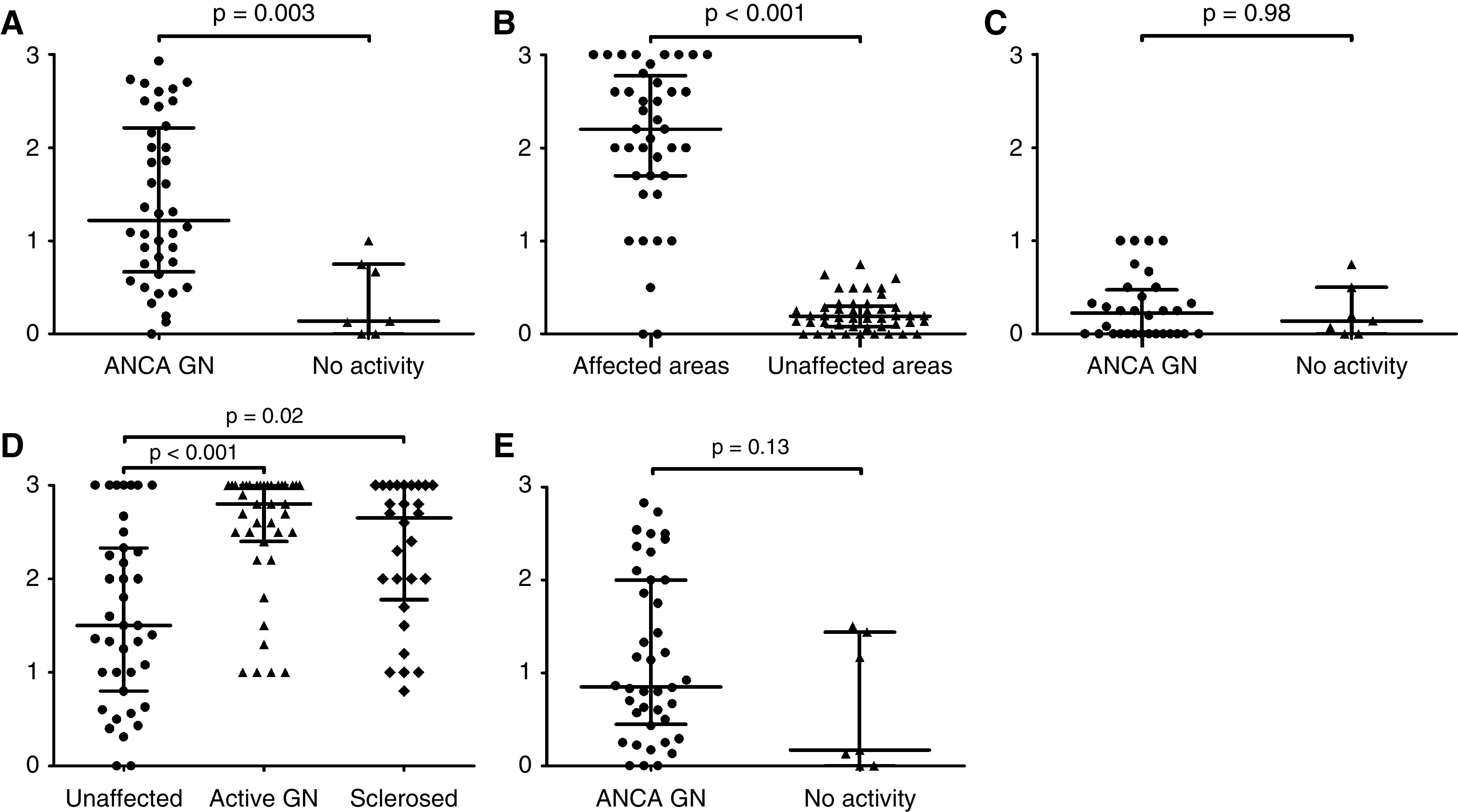
Results: High levels of urinary soluble CD163 were found in 96 (87%) of 110 biopsies with active ANCA-associated GN compared with one (7%) of 15 biopsies without active ANCA-associated GN and one (6%) of 17 healthy controls. Urinary soluble CD163 correlated with fibrinoid necrosis (Rho=0.48, P<0.001) and cellular crescents (Rho=0.70, P<0.001) on kidney biopsy. In repeated biopsies, urinary soluble CD163's sensitivity of 0.94 and specificity of 0.91 for the recognition of relapsing ANCA-associated GN appeared better than routine clinical measures. The presence of CD163+ cells in affected glomeruli confirmed urinary soluble CD163's origin.
Conclusions: Urinary soluble CD163 is associated with active ANCA-associated GN and correlates with histologic features as seen in ANCA-associated GN.
Podcast: This article contains a podcast at https://www.asn-online.org/media/podcast/CJASN/2020_11_17_CJN07210520_final.mp3.
Keywords: ANCA; Acute kidney injury; Biopsy; glomerulonephritis; kidney biopsy; kidney pathology; macrophages; vasculitis.
Copyright © 2020 by the American Society of Nephrology.
Figures
References
-
- Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, Flores-Suarez LF, Gross WL, Guillevin L, Hagen EC, Hoffman GS, Jayne DR, Kallenberg CG, Lamprecht P, Langford CA, Luqmani RA, Mahr AD, Matteson EL, Merkel PA, Ozen S, Pusey CD, Rasmussen N, Rees AJ, Scott DG, Specks U, Stone JH, Takahashi K, Watts RA: 2012 revised International Chapel Hill Consensus Conference nomenclature of vasculitides. Arthritis Rheum 65: 1–11, 2013. - PubMed
-
- van Paassen P, van Breda Vriesman PJ, van Rie H, Tervaert JW: Signs and symptoms of thin basement membrane nephropathy: A prospective regional study on primary glomerular disease-The Limburg Renal Registry. Kidney Int 66: 909–913, 2004. - PubMed
-
- Berden AE, Ferrario F, Hagen EC, Jayne DR, Jennette JC, Joh K, Neumann I, Noël LH, Pusey CD, Waldherr R, Bruijn JA, Bajema IM: Histopathologic classification of ANCA-associated glomerulonephritis. J Am Soc Nephrol 21: 1628–1636, 2010. - PubMed
-
- Moiseev S, Novikov P, Jayne D, Mukhin N: End-stage renal disease in ANCA-associated vasculitis. Nephrol Dial Transplant 32: 248–253, 2017. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
