Implementation of Venoarterial Extracorporeal Membrane Oxygenation in Nonintubated Patients
- PMID: 33203803
- PMCID: PMC7946527
- DOI: 10.5090/kjtcs.20.070
Implementation of Venoarterial Extracorporeal Membrane Oxygenation in Nonintubated Patients
Abstract
Background: Although extracorporeal membrane oxygenation (ECMO) is generally performed percutaneously, the technology is deployed under sedation and necessitates endotracheal intubation. However, in some patients, the use of venoarterial (VA) ECMO without intubation may be beneficial. Herein, we describe our experiences with VA ECMO performed without prior endotracheal intubation.
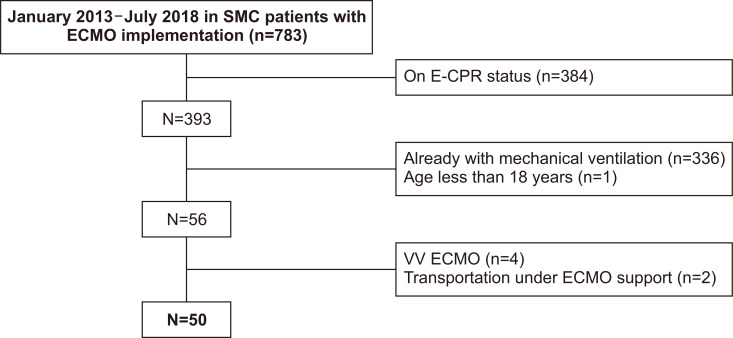
Methods: A total of 783 patients treated with VA ECMO at a single center between January 2013 and July 2018 were reviewed retrospectively. We included patients who underwent successful VA ECMO implementation without prior endotracheal intubation, and excluded those who were younger than 18 years, had ongoing cardiopulmonary resuscitation status, and had poor quality of the vessels needed for percutaneous cannulation. The primary study outcome was in-hospital survival.
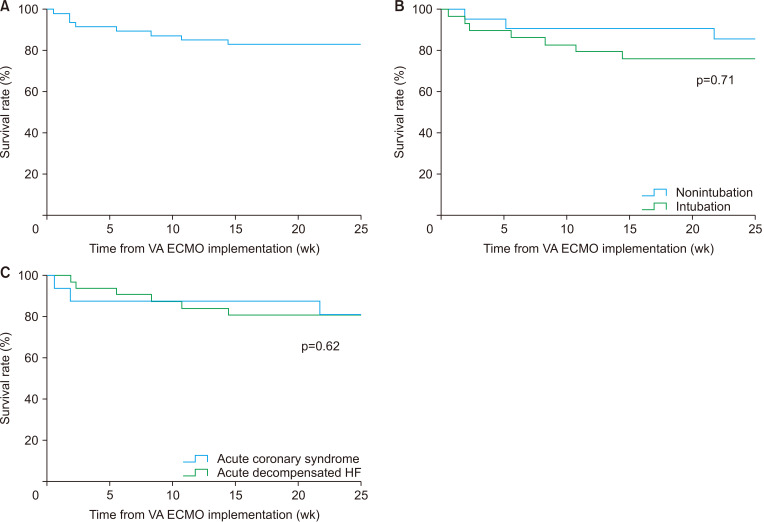
Results: In total, 50 patients were included in this study, 94% of whom showed cardiogenic shock. The mean age of the study participants was 56.3±14.5 years. The median VA ECMO support time was 7 days (range, 2-13 days). Twenty-one patients (42%) did not receive ventilator care during the VA ECMO support period, while 29 patients (58%) progressed to intubation after VA ECMO implementation. The rates of survival at discharge and weaning success were 82% (n=41) and 92% (n=46), respectively, and 80% (n=40) of patients presented good Glasgow-Pittsburgh Cerebral Performance Categories scores at discharge.
Conclusion: Even in patients with cardiogenic shock, percutaneous VA ECMO can be introduced safely without prior endotracheal intubation by an experienced care team. The application of nonintubated VA ECMO might be a feasible strategy in selected cases.
Keywords: Endotracheal; Extracorporeal membrane oxygenation; Intubation.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures

References
-
- Strieter RM, Lynch JP., 3rd Complications in the ventilated patient. Clin Chest Med. 1988;9:127–39. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources