

Resistance and Overcoming Resistance in Breast Cancer
- PMID: 33204149
- PMCID: PMC7666993
- DOI: 10.2147/BCTT.S270799
Resistance and Overcoming Resistance in Breast Cancer
Abstract
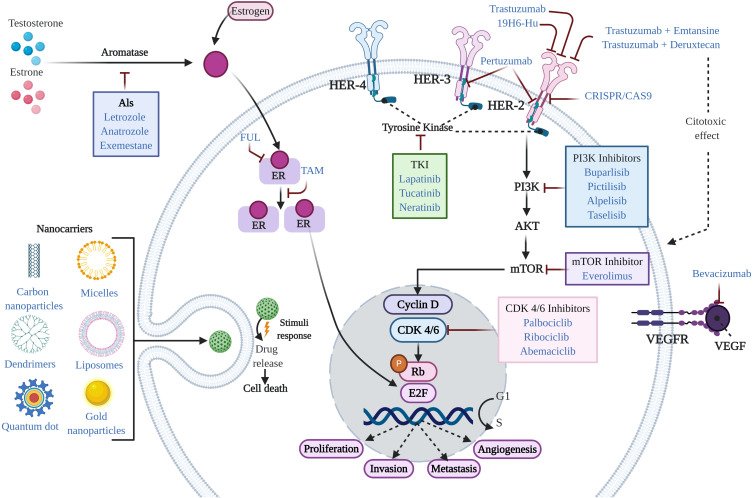
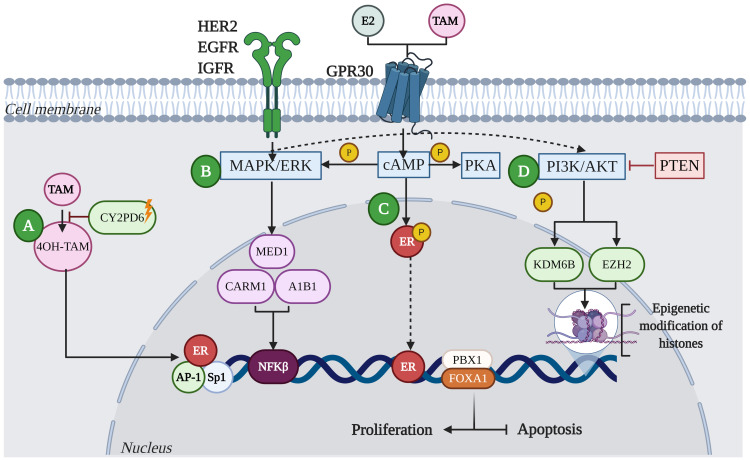
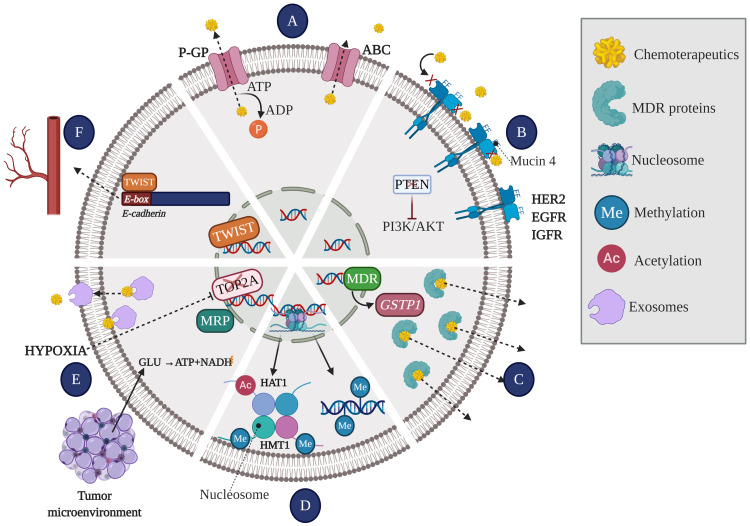
The incidence and mortality of breast cancer (BC) have increased in recent years, and BC is the main cause of cancer-related death in women worldwide. One of the most significant clinical problems in the treatment of patients with BC is the development of therapeutic resistance. Therefore, elucidating the molecular mechanisms involved in drug resistance is critical. The therapeutic decision for the management of patients with BC is based not only on the assessment of prognostic factors but also on the evaluation of clinical and pathological parameters. Although this has been a successful approach, some patients relapse and/or eventually develop resistance to treatment. This review is focused on recent studies on the possible biological and molecular mechanisms involved in both response and resistance to treatment in BC. Additionally, emerging treatments that seek to overcome resistance and reduce side effects are also described. A greater understanding of the mechanisms of action of treatments used in BC might contribute not only to the enhancement of our understanding of the mechanisms involved in the development of resistance but also to the optimization of the existing treatment regimens.
Keywords: breast cancer; chemotherapy; emerging treatments; endocrine therapy; resistance.
© 2020 Luque-Bolivar et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
References
-
- International Agency for Research on Cancer. Global cancer observatory. Cancer Today; 2018. Available from: https://gco.iarc.fr/. Accessed November3, 2020.
-
- International Agency for Research on Cancer. Global cancer observatory. Latest world cancer statistics – GLOBOCAN 2012: estimated cancer incidence, mortality and prevalence Worldwide in 2012; 2013. Available from: https://www.iarc.fr/news-events/latest-world-cancer-statistics-globocan-.... Accessed November3, 2020.
Publication types
LinkOut - more resources
Full Text Sources
