

Trends in the treatment of infected knee arthroplasty
- PMID: 33204510
- PMCID: PMC7608567
- DOI: 10.1302/2058-5241.5.190069
Trends in the treatment of infected knee arthroplasty
Abstract
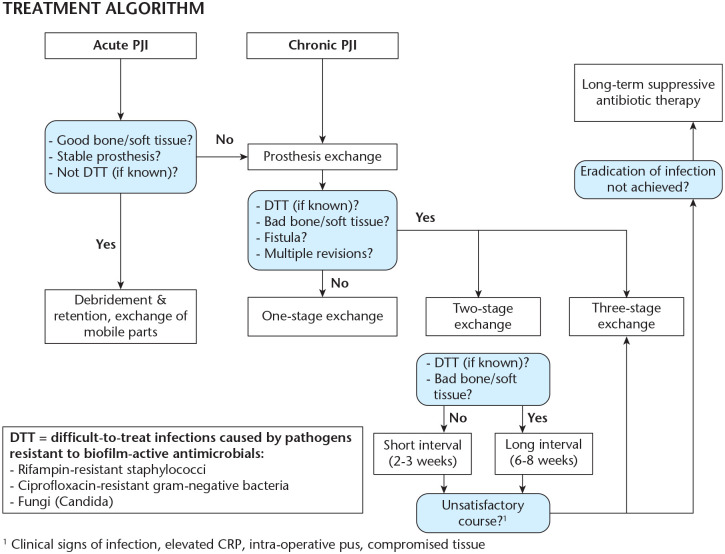
Essential treatment methods for infected knee arthroplasty involve DAIR (debridement, antibiotics, and implant retention), and one and two-stage exchange arthroplasty.Aggressive debridement with the removal of all avascular tissues and foreign materials that contain biofilm is mandatory for all surgical treatment modalities.DAIR is a viable option with an acceptable success rate and can be used as a first surgical procedure for patients who have a well-fixed, functioning prosthesis without a sinus tract for acute-early or late-hematogenous acute infections with no more than four weeks (most favourable being < seven days) of symptoms. Surgeons must focus on the isolation of the causative organism with sensitivities to bactericidal treatment as using one-stage exchange.One-stage exchange is indicated when the patients have:minimal bone loss/soft tissue defect allowing primary wound closure,easy to treat micro-organisms,absence of systemic sepsis andabsence of extensive comorbidities.There are no validated serum or synovial biomarkers to determine optimal timing of re-implantation for two-stage exchange.Antibiotic-free waiting intervals and joint aspiration before the second stage are no longer recommended. The decision to perform aspiration should be made based on the index of suspicion for persistent infection.Re-implantation can be performed when the treating medical team feels that the clinical signs of infection are under control and serological tests are trending downwards. Cite this article: EFORT Open Rev 2020;5:672-683. DOI: 10.1302/2058-5241.5.190069.
Keywords: infected total knee arthroplasty; periprosthetic infection; trends.
© 2020 The author(s).
Conflict of interest statement
ICMJE Conflict of interest statement: IRT reports consultancy, payments for lectures including service on speakers’ bureaus, and royalties from Smith & Nephew outside the submitted work. The other authors declare no conflict of interest relevant to this work.
Figures

References
-
- Gehrke T, Alijanipour P, Parvizi J. The management of an infected total knee arthroplasty. Bone Joint J 2015;97-B:20–29. - PubMed
-
- Kurtz SM, Lau E, Schmier J, Ong KL, Zhao K, Parvizi J. Infection burden for hip and knee arthroplasty in the United States. J Arthroplasty 2008;23:984–991. - PubMed
-
- Gomez-Urena EO, Tande AJ, Osmon DR, Berbari EF. Diagnosis of prosthetic joint infection: cultures, biomarker and criteria. Infect Dis Clin North Am 2017;31:219–235. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
