

Needle in a haystack: Robotic removal of a retroperitoneal wire
- PMID: 33204640
- PMCID: PMC7649612
- DOI: 10.1016/j.eucr.2020.101472
Needle in a haystack: Robotic removal of a retroperitoneal wire
Abstract
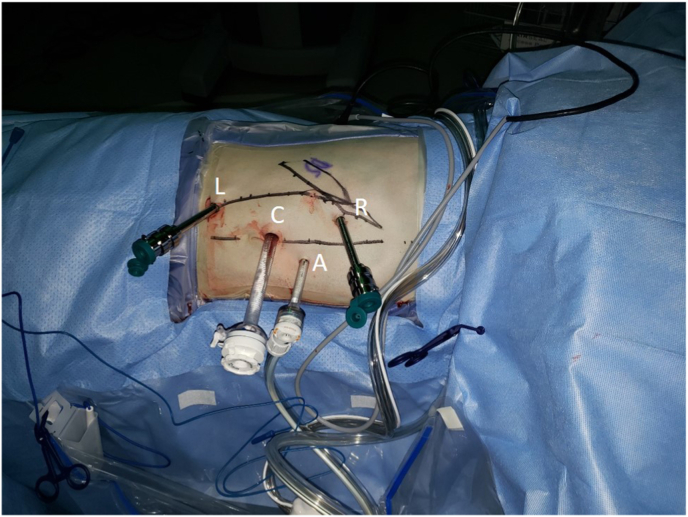
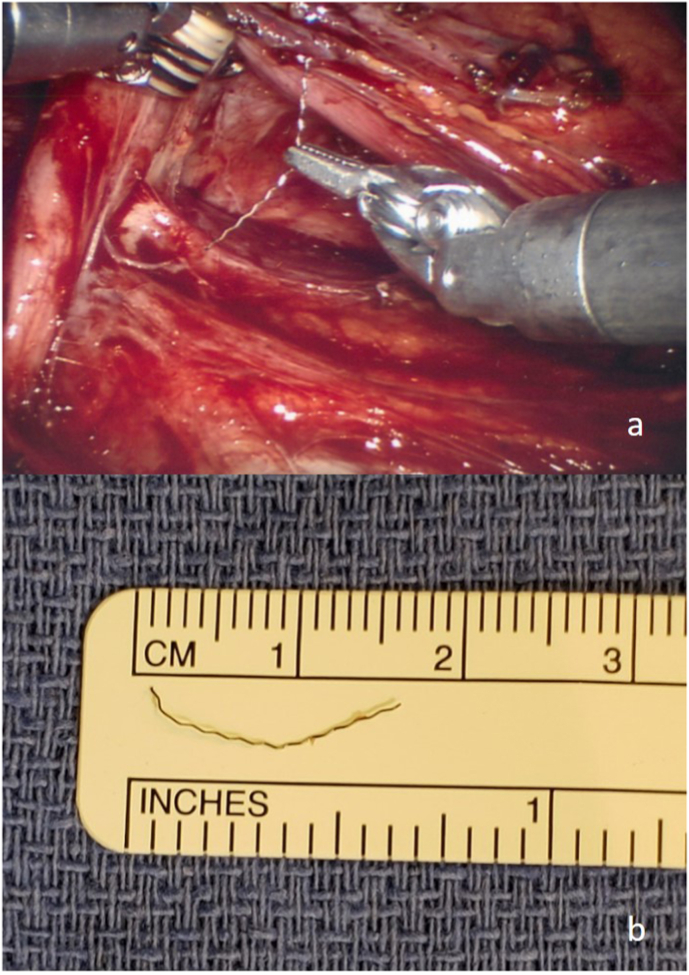
Retroperitoneal foreign bodies are rare indications for exploratory surgery. We present a case of a 19-year-old male with abdominal pain after a fall who was found to have a linear metallic object adjacent to the right ureter and inferior vena cava. Given the patient's pain and discomfort, he elected for robotic exploration of the retroperitoneum, which was carried out successfully with the Da Vinci Si® robot. This case demonstrates the feasibility of robotic retroperitoneal exploration and foreign body retrieval for a very small object.
Keywords: Robotic; foreign body; retroperitoneal.
© 2020 Published by Elsevier Inc.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
