

Hemangiopericytoma: Incidence, Treatment, and Prognosis Analysis Based on SEER Database
- PMID: 33204688
- PMCID: PMC7655240
- DOI: 10.1155/2020/2468320
Hemangiopericytoma: Incidence, Treatment, and Prognosis Analysis Based on SEER Database
Abstract
Background: Hemangiopericytomas are rare tumors derived from pericytes surrounding the blood vessels. The clinicopathological characteristics and prognosis of hemangiopericytoma patients remain mostly unknown. In this retrospective cohort study, we assessed the clinicopathological characteristics of hemangiopericytoma patients, as well as the clinical usefulness of different treatment modalities. Material and Methods. We collected the clinicopathological data (between 1975 and 2016) of hemangiopericytoma and hemangioendothelioma patients from the Surveillance, Epidemiology, and End Results (SEER) database. Incidence, treatment, and patient prognosis were assessed.
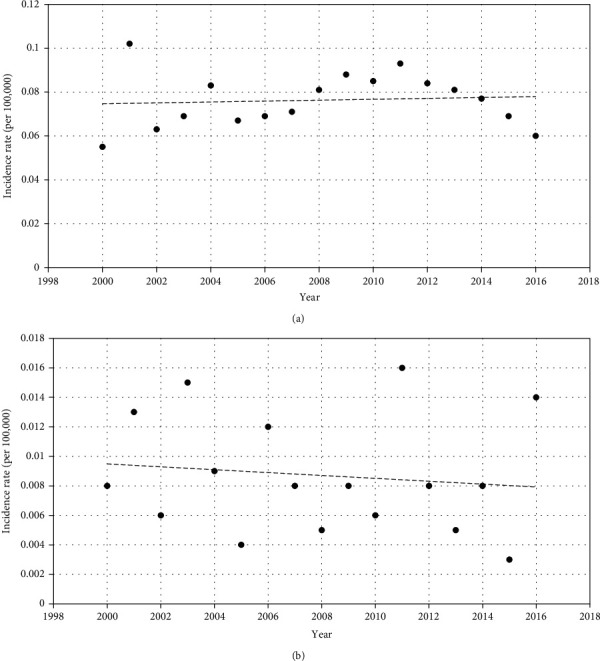
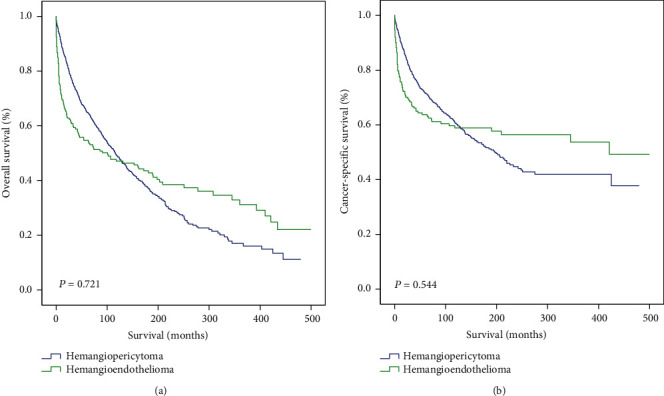
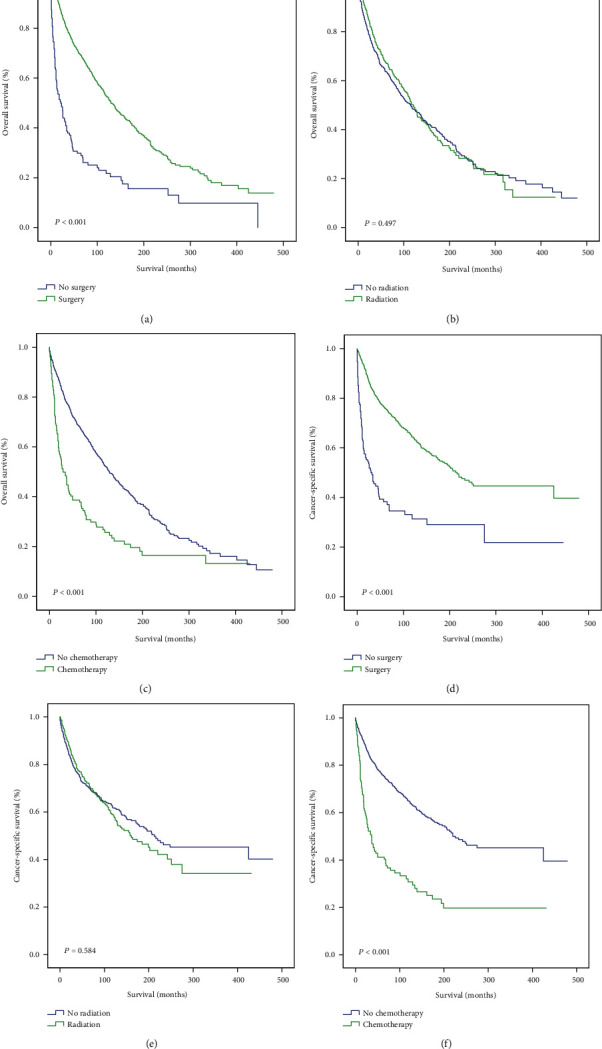
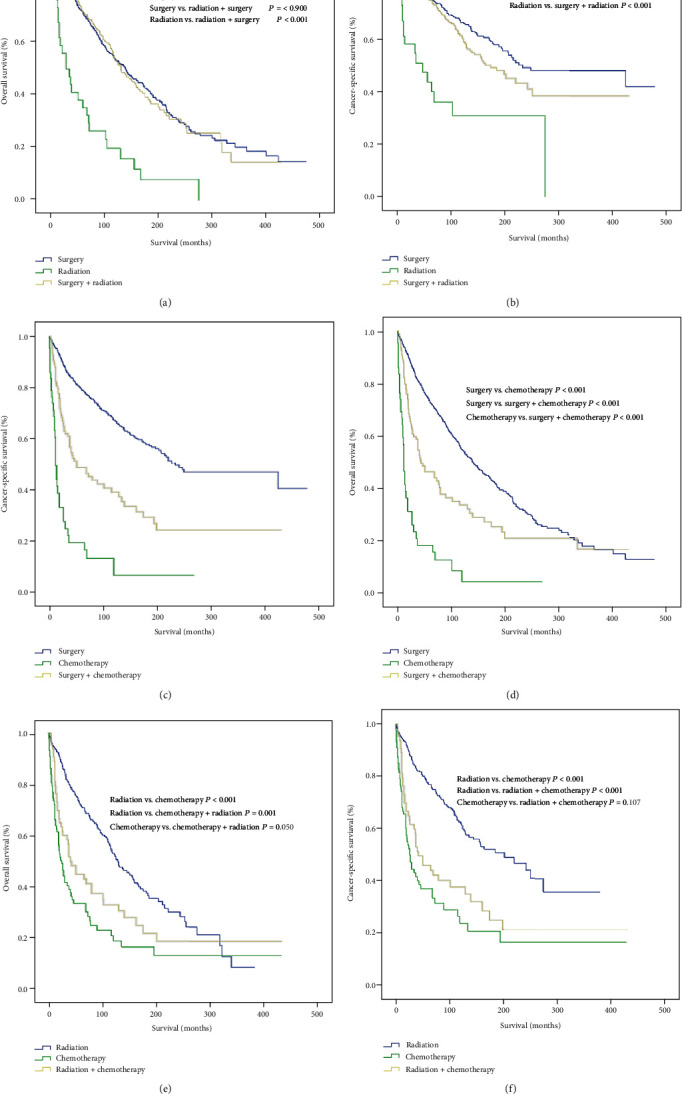
Results: Data from 1474 patients were analyzed in our study cohort (hemangiopericytoma: n = 1243; hemangioendothelioma: n = 231). The incidence of hemangiopericytoma in 2016 was 0.060 per 100,000 individuals. The overall survival (OS) and cancer-specific survival (CSS) did not differ between patients with hemangioendothelioma and those with hemangiopericytoma (P = 0.721, P = 0.544). The tumor grade had no effect on the OS of hemangiopericytoma patients. Multivariate analysis revealed the clinical usefulness of surgery in hemangiopericytoma patients (HR = 0.15, 95% confidence interval: 0.05-0.41, P < 0.001). In contrast, radiotherapy did not improve OS (P = 0.497) or CSS (P = 0.584), and chemotherapy worsened patient survival (P < 0.001). Additionally, the combination of surgery and radiotherapy had a similar effect with surgery alone on hemangiopericytoma patient survival (OS: P = 0.900; CSS: P = 0.156). Surgery plus chemotherapy provided a worse clinical benefit than surgery alone (P < 0.001).
Conclusions: Our findings suggested that hemangiopericytoma had a similar prognosis with hemangioendothelioma. Surgery was the only effective treatment that provided survival benefits in hemangiopericytoma patients, while the clinical usefulness of adjuvant chemotherapy or radiotherapy was limited.
Copyright © 2020 Kewei Wang et al.
Conflict of interest statement
There is no potential conflict of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
