

Randomized comparison of oesophageal protection with a temperature control device: results of the IMPACT study
- PMID: 33205201
- PMCID: PMC7868886
- DOI: 10.1093/europace/euaa276
Randomized comparison of oesophageal protection with a temperature control device: results of the IMPACT study
Abstract
Aims: Thermal injury to the oesophagus is an important cause of life-threatening complication after ablation for atrial fibrillation (AF). Thermal protection of the oesophageal lumen by infusing cold liquid reduces thermal injury to a limited extent. We tested the ability of a more powerful method of oesophageal temperature control to reduce the incidence of thermal injury.
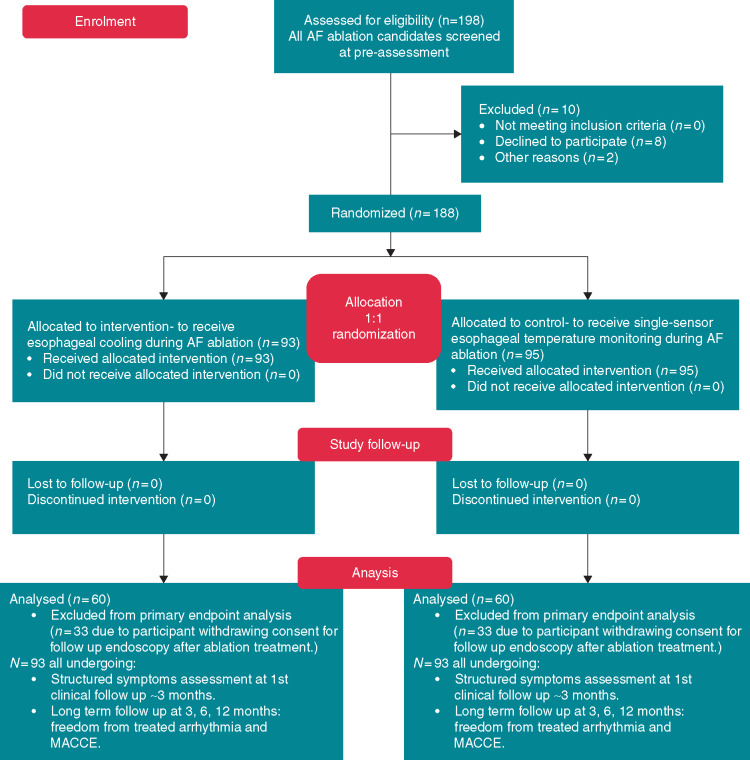
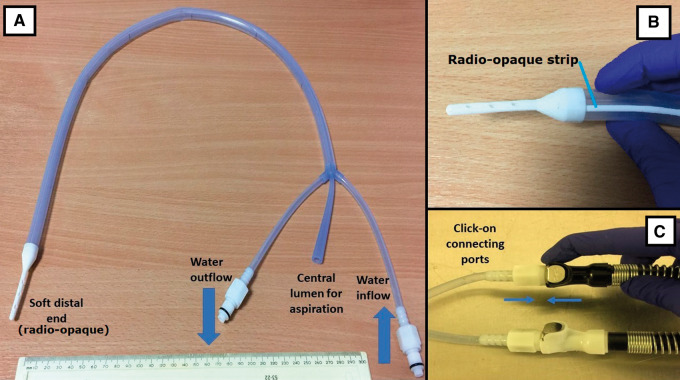
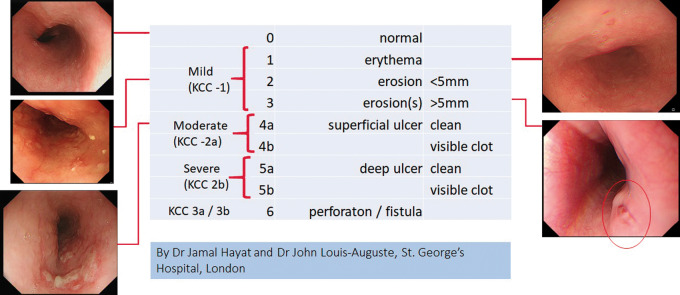
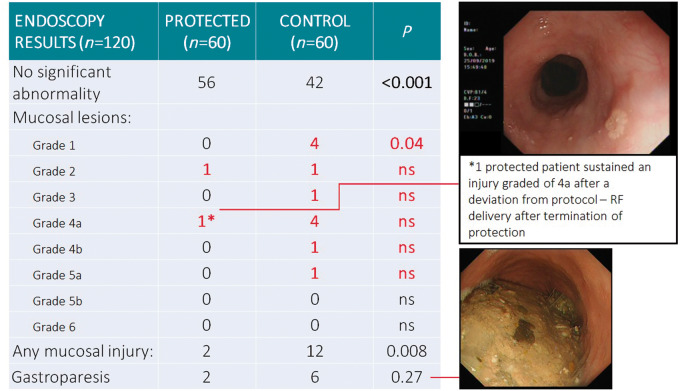
Methods and results: A single-centre, prospective, double-blinded randomized trial was used to investigate the ability of the ensoETM device to protect the oesophagus from thermal injury. This device was compared in a 1:1 randomization with a control group of standard practice utilizing a single-point temperature probe. In the protected group, the device maintained the luminal temperature at 4°C during radiofrequency (RF) ablation for AF under general anaesthesia. Endoscopic examination was performed at 7 days post-ablation and oesophageal injury was scored. The patient and the endoscopist were blinded to the randomization. We recruited 188 patients, of whom 120 underwent endoscopy. Thermal injury to the mucosa was significantly more common in the control group than in those receiving oesophageal protection (12/60 vs. 2/60; P = 0.008), with a trend toward reduction in gastroparesis (6/60 vs. 2/60, P = 0.27). There was no difference between groups in the duration of RF or in the force applied (P value range= 0.2-0.9). Procedure duration and fluoroscopy duration were similar (P = 0.97, P = 0.91, respectively).
Conclusion: Thermal protection of the oesophagus significantly reduces ablation-related thermal injury compared with standard care. This method of oesophageal protection is safe and does not compromise the efficacy or efficiency of the ablation procedure.
Keywords: Atrial fibrillation; Atrio-oesophageal fistula; Catheter ablation; Gastroparesis; Oesophagus; Temperature control.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Kapur S, Barbhaiya C, Deneke T, Michaud GF.. Esophageal injury and atrioesophageal fistula caused by ablation for atrial fibrillation. Circulation 2017;136:1247–55. - PubMed
-
- Miyazaki S, Nakamura H, Taniguchi H, Takagi T, Iwasawa J, Watanabe T. et al. Esophagus-related complications during second-generation cryoballoon ablation—insight from simultaneous esophageal temperature monitoring from 2 esophageal probes. J Cardiovasc Electrophysiol 2016;27:1038–44. - PubMed
-
- Schmidt M, Nolker G, Marschang H, Gutleben KJ, Schibgilla V, Rittger H. et al. Incidence of oesophageal wall injury post-pulmonary vein antrum isolation for treatment of patients with atrial fibrillation. Europace 2008;10:205–9. - PubMed
-
- Lakkireddy D, Reddy YM, Atkins D, Rajasingh J, Kanmanthareddy A, Olyaee M. et al. Effect of atrial fibrillation ablation on gastric motility: the atrial fibrillation gut study. Circ Arrhythm Electrophysiol 2015;8:531–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
