

Characterization of Sentinel Lymph Node Immune Signatures and Implications for Risk Stratification for Adjuvant Therapy in Melanoma
- PMID: 33205334
- PMCID: PMC8126577
- DOI: 10.1245/s10434-020-09277-w
Characterization of Sentinel Lymph Node Immune Signatures and Implications for Risk Stratification for Adjuvant Therapy in Melanoma
Abstract
Background: Although sentinel lymph node (SLN) biopsy is a standard procedure used to identify patients at risk for melanoma recurrence, it fails to risk-stratify certain patients accurately. Because processes in SLNs regulate anti-tumor immune responses, the authors hypothesized that SLN gene expression may be used for risk stratification.
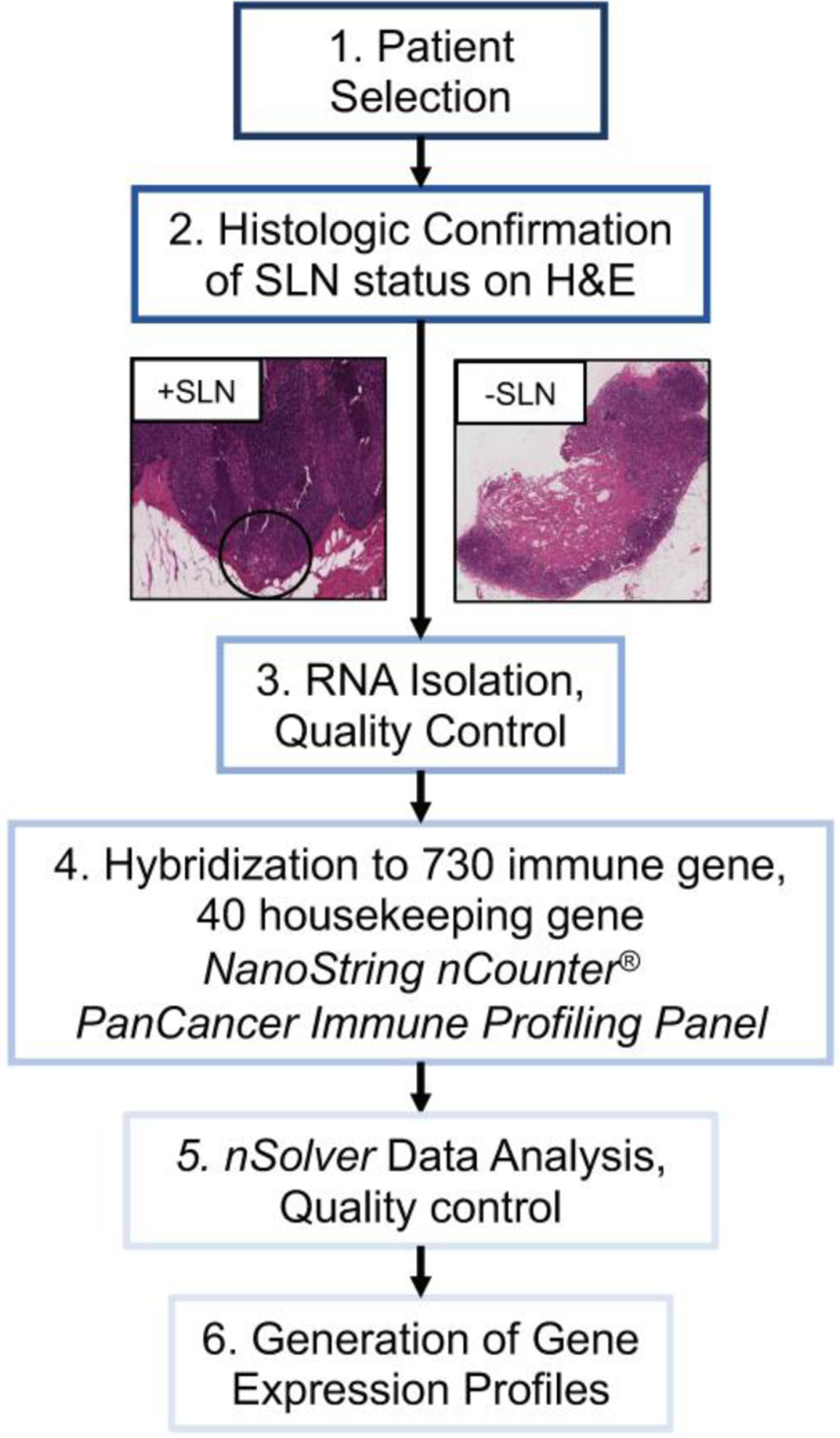
Methods: The Nanostring nCounter PanCancer Immune Profiling Panel was used to quantify expression of 730 immune-related genes in 60 SLN specimens (31 positive [pSLNs], 29 negative [nSLNs]) from a retrospective melanoma cohort. A multivariate prediction model for recurrence-free survival (RFS) was created by applying stepwise variable selection to Cox regression models. Risk scores calculated on the basis of the model were used to stratify patients into low- and high-risk groups. The predictive power of the model was assessed using the Kaplan-Meier and log-rank tests.
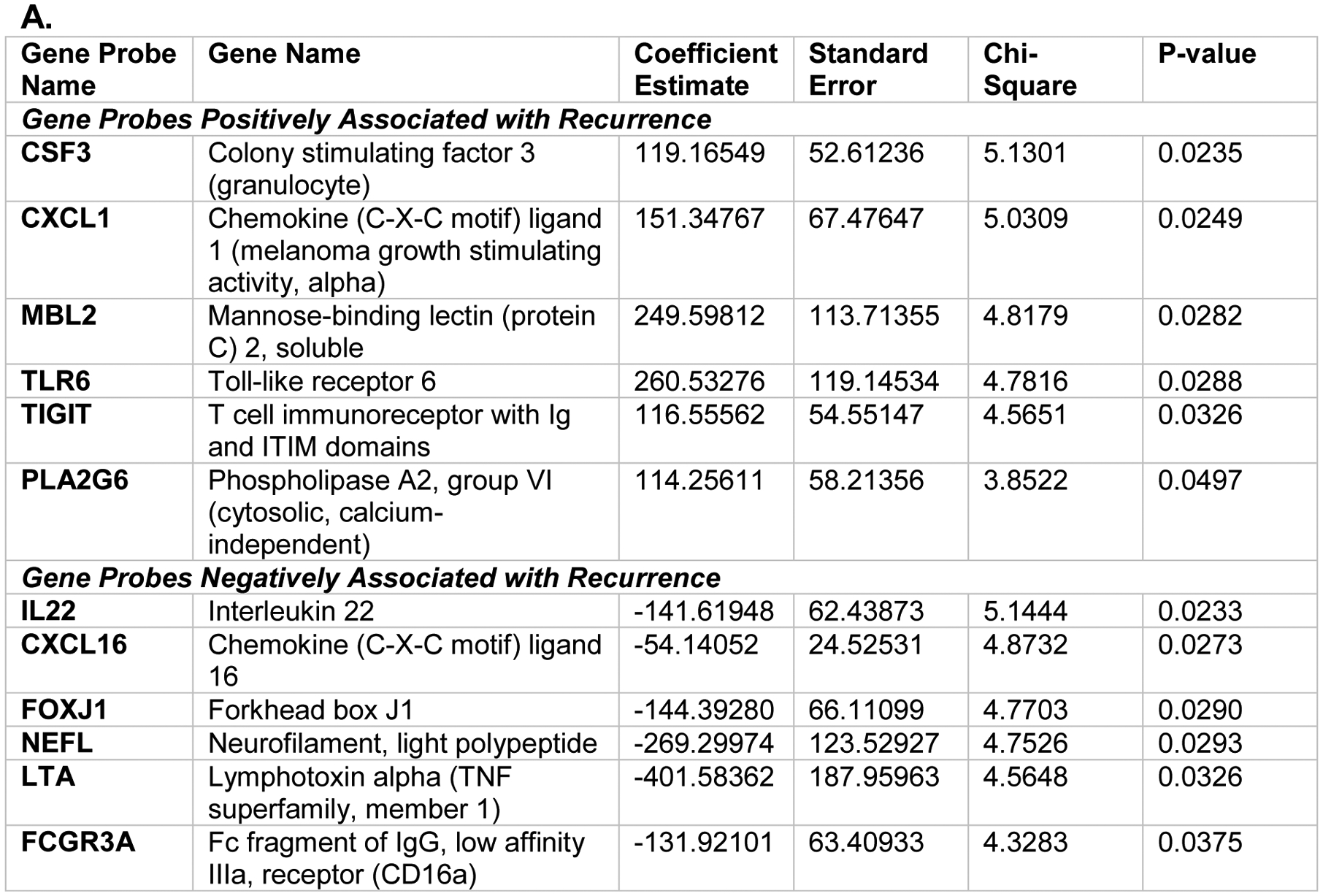
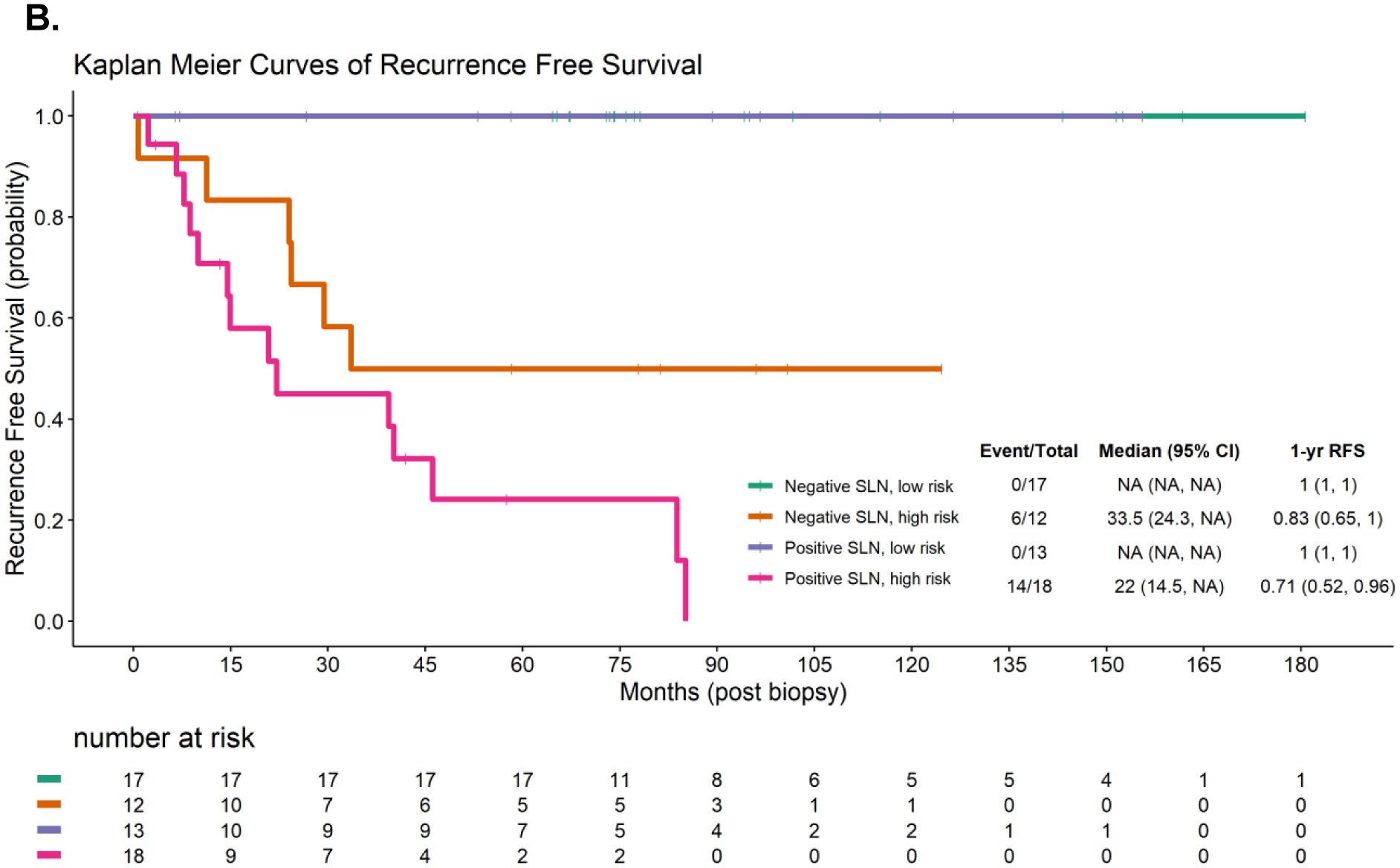
Results: During a median follow-up period of 6.3 years, 20 patients (33.3%) experienced recurrence (pSLN, 45.2% [14/31] vs nSLN, 20.7% [6/29]; p = 0.0445). A fitted Cox regression model incorporating 12 genes accurately predicted RFS (C-index, 0.9919). Improved RFS was associated with increased expression of TIGIT (p = 0.0326), an immune checkpoint, and decreased expression of CXCL16 (p = 0.0273), a cytokine important in promoting dendritic and T cell interactions. Independent of SLN status, the model in this study was able to stratify patients into cohorts at high and low risk for recurrence (p < 0.001, log-rank).
Conclusions: Expression profiles of the SLN gene are associated with melanoma recurrence and may be able to identify patients as high or low risk regardless of SLN status, potentially enhancing patient selection for adjuvant therapy.
Figures
References
-
- Thomas DC, Han G, Leong SP, et al. Recurrence of Melanoma After a Negative Sentinel Node Biopsy: Predictors and Impact of Recurrence Site on Survival. Annals of surgical oncology. 2019;26(7):2254–2262. - PubMed
-
- Landow SM, Gjelsvik A, Weinstock MA. Mortality burden and prognosis of thin melanomas overall and by subcategory of thickness, SEER registry data, 1992–2013. Journal of the American Academy of Dermatology. 2017;76(2):258–263. - PubMed
-
- Eggermont AMM, Dummer R. The 2017 complete overhaul of adjuvant therapies for high-risk melanoma and its consequences for staging and management of melanoma patients. European journal of cancer (Oxford, England : 1990). 2017;86:101–105. - PubMed
-
- Eggermont AMM, Blank CU, Mandala M, et al. Adjuvant Pembrolizumab versus Placebo in Resected Stage III Melanoma. N Engl J Med. 2018;378(19):1789–1801. - PubMed
-
- Weber J, Mandala M, Del Vecchio M, et al. Adjuvant Nivolumab versus Ipilimumab in Resected Stage III or IV Melanoma. N Engl J Med. 2017;377(19):1824–1835. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
