

Phenotypes and personalized medicine in the acute respiratory distress syndrome
- PMID: 33206201
- PMCID: PMC7673253
- DOI: 10.1007/s00134-020-06296-9
Phenotypes and personalized medicine in the acute respiratory distress syndrome
Abstract
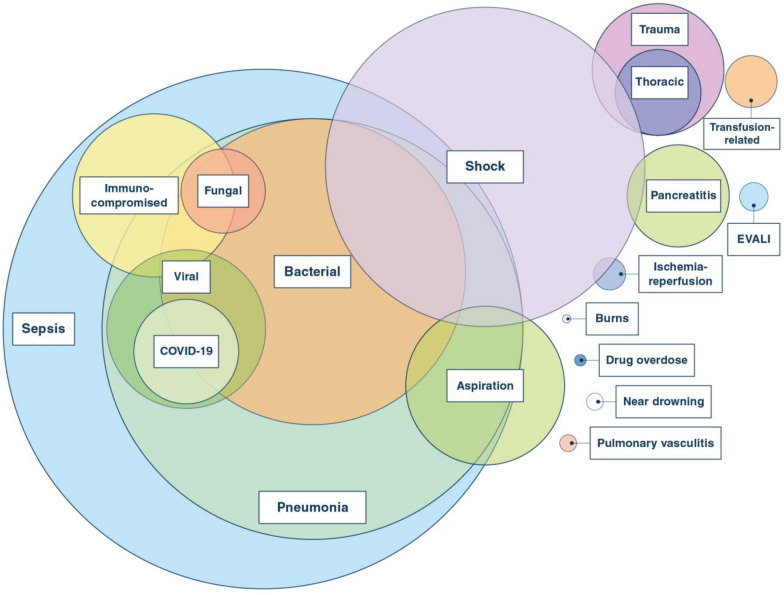
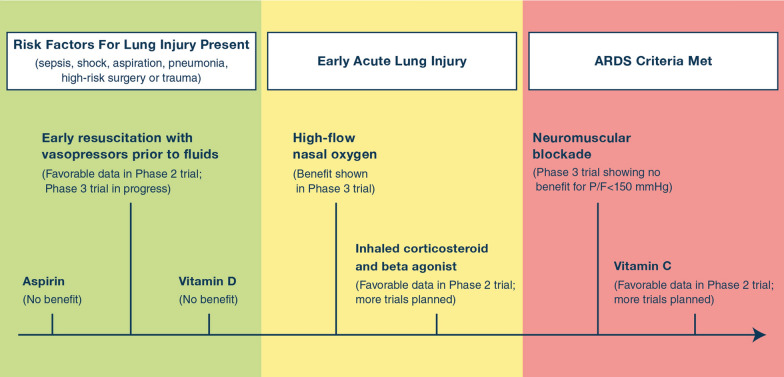
Although the acute respiratory distress syndrome (ARDS) is well defined by the development of acute hypoxemia, bilateral infiltrates and non-cardiogenic pulmonary edema, ARDS is heterogeneous in terms of clinical risk factors, physiology of lung injury, microbiology, and biology, potentially explaining why pharmacologic therapies have been mostly unsuccessful in treating ARDS. Identifying phenotypes of ARDS and integrating this information into patient selection for clinical trials may increase the chance for efficacy with new treatments. In this review, we focus on classifying ARDS by the associated clinical disorders, physiological data, and radiographic imaging. We consider biologic phenotypes, including plasma protein biomarkers, gene expression, and common causative microbiologic pathogens. We will also discuss the issue of focusing clinical trials on the patient's phase of lung injury, including prevention, administration of therapy during early acute lung injury, and treatment of established ARDS. A more in depth understanding of the interplay of these variables in ARDS should provide more success in designing and conducting clinical trials and achieving the goal of personalized medicine.
Keywords: Acute lung injury; Acute respiratory distress syndrome; COVID-19; Phenotype; Precision medicine; Pulmonary edema; Sepsis.
Conflict of interest statement
The authors have no conflicts of interest for this manuscript.
Figures

References
-
- Beigel JH, Tomashek KM, Dodd LE, Mehta AK, Zingman BS, Kalil AC, Hohmann E, Chu HY, Luetkemeyer A, Kline S, Lopez de Castilla D, Finberg RW, Dierberg K, Tapson V, Hsieh L, Patterson TF, Paredes R, Sweeney DA, Short WR, Touloumi G, Lye DC, Ohmagari N, Oh MD, Ruiz-Palacios GM, Benfield T, Fatkenheuer G, Kortepeter MG, Atmar RL, Creech CB, Lundgren J, Babiker AG, Pett S, Neaton JD, Burgess TH, Bonnett T, Green M, Makowski M, Osinusi A, Nayak S, Lane HC, Members A-SG, (2020) Remdesivir for the Treatment of Covid-19 - Final Report. N Engl J Med - PMC - PubMed
-
- Guerin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, Mercier E, Badet M, Mercat A, Baudin O, Clavel M, Chatellier D, Jaber S, Rosselli S, Mancebo J, Sirodot M, Hilbert G, Bengler C, Richecoeur J, Gainnier M, Bayle F, Bourdin G, Leray V, Girard R, Baboi L, Ayzac L, Group PS Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368:2159–2168. - PubMed
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley DF, Ranieri M, Rubenfeld G, Thompson BT, Wrigge H, Slutsky AS, Pesenti A, LS Investigators, Group ET Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315:788–800. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HL134828/NH/NIH HHS/United States
- 5TL1TR001871-05/NH/NIH HHS/United States
- R01 HL126176/HL/NHLBI NIH HHS/United States
- R35 HL140026/HL/NHLBI NIH HHS/United States
- K23 HL133489/NH/NIH HHS/United States
- U01 HL123004/HL/NHLBI NIH HHS/United States
- HL126176/National Institutes of Health (US)/International
- UH3HL141736/GF/NIH HHS/United States
- HL140026/National Institutes of Health (US)/International
- 5T32GM008440-24/National Institutes of Health (US)/International
- UH3 HL141736/HL/NHLBI NIH HHS/United States
- HL14722/NH/NIH HHS/United States
- R21 HL145506/HL/NHLBI NIH HHS/United States
- HL145506/NH/NIH HHS/United States
- HL123004/NH/NIH HHS/United States
- TL1 TR001871/TR/NCATS NIH HHS/United States
- R01 HL134828/HL/NHLBI NIH HHS/United States
- K23 HL133489/HL/NHLBI NIH HHS/United States
- T32 GM008440/GM/NIGMS NIH HHS/United States
- 140026/National Institutes of Health (US)/International
