

Adsorption therapy in critically ill with septic shock and acute kidney injury: a retrospective and prospective cohort study
- PMID: 33206229
- PMCID: PMC7672170
- DOI: 10.1186/s13613-020-00772-7
Adsorption therapy in critically ill with septic shock and acute kidney injury: a retrospective and prospective cohort study
Abstract
Background: Haemoadsorption has been described as an effective way to control increased pro- and anti-inflammatory mediators ("cytokine storm") in septic shock patients. No prospective or randomised clinical study has yet confirmed these results. However, no study has yet prospectively specifically investigated patients in severe septic shock with sepsis-associated acute kidney injury (SA-AKI). Therefore, we aimed to examine whether haemoadsorption could influence intensive care unit (ICU) and hospital mortality in these patients. Furthermore, we examined the influence of haemoadsorption on length of stay in the ICU and therapeutic support.
Methods: Retrospective control group and prospective intervention group design in a tertiary hospital in central Europe (Germany). Intervention was the implementation of haemoadsorption for patients in septic shock with SA-AKI. 76 patients were included in this analysis.
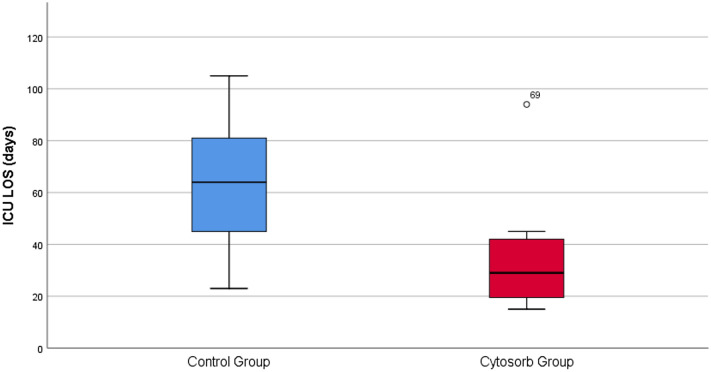
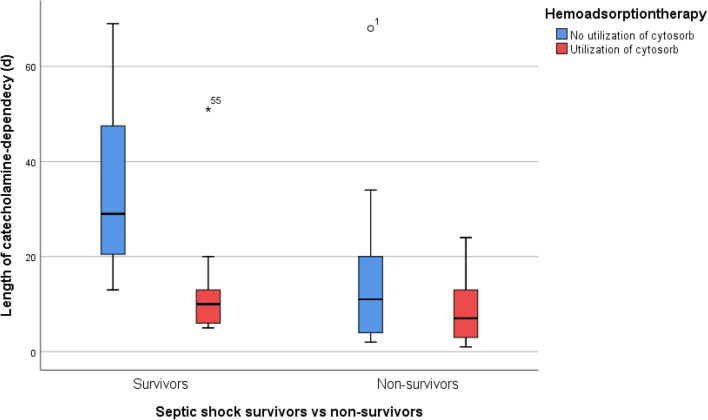
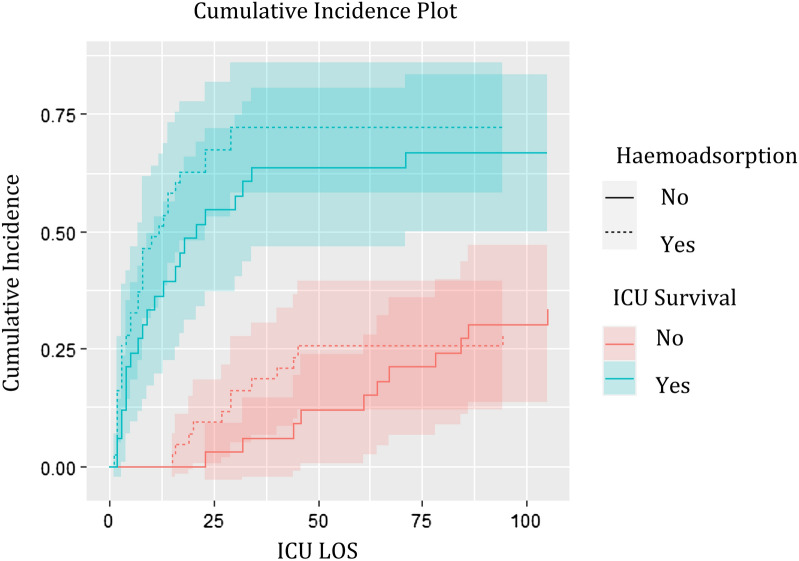
Results: Severity of illness as depicted by APACHE II was higher in patients treated with haemoadsorption. Risk-adjusted ICU mortality rates (O/E ratios) did not differ significantly between the groups (0.80 vs. 0.83). We observed in patients treated with haemoadsorption a shorter LOS and shorter therapeutic support such as catecholamine dependency and duration of RRT. However, in multivariate analysis (logistic regression for mortality, competing risk for LOS), we found no significant differences between the two groups.
Conclusions: The implementation of haemoadsorption for patients in septic shock with acute renal failure did not lead to a reduction in ICU or hospital mortality rates. Despite univariate analysis delivering some evidence for a shorter duration of ICU-related treatments in the haemoadsorption group, these results did not remain significant in multivariate analysis. Trial registration CytoSorb® registry https://clinicaltrials.gov/ct2/show/NCT02312024 . December 9, 2014.
Database: https://www.cytosorb-registry.org/ (registration for content acquisition is necessary).
Keywords: Acute kidney injury; Cytosorb; Haemoadsorption; Mortality; Outcome; Sepsis; Septic shock.
Conflict of interest statement
GAS has received financial travel support for attending a symposium organised by CytoSorbents Europe GmbH in 2016. All other authors declare that there are no potential conflicts of interest to disclose.
Figures
Similar articles
-
Impact of Haemoadsorption Therapy on Short Term Mortality and Vasopressor Dependency in Severe Septic Shock with Acute Kidney Injury: A Retrospective Cohort Study.Antibiotics (Basel). 2024 Dec 22;13(12):1233. doi: 10.3390/antibiotics13121233. Antibiotics (Basel). 2024. PMID: 39766623 Free PMC article.
-
[Clinical characteristics and prognosis of acute kidney injury in elderly patients with sepsis].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019 Jul;31(7):837-841. doi: 10.3760/cma.j.issn.2095-4352.2019.07.008. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019. PMID: 31441406 Chinese.
-
Multicentered prospective investigator initiated study to evaluate the clinical outcomes with extracorporeal cytokine adsorption device (CytoSorb®) in patients with sepsis and septic shock.World J Crit Care Med. 2021 Jan 9;10(1):22-34. doi: 10.5492/wjccm.v10.i1.22. eCollection 2021 Jan 9. World J Crit Care Med. 2021. PMID: 33505870 Free PMC article.
-
Renal Replacement Techniques in Septic Shock.Int J Mol Sci. 2021 Sep 23;22(19):10238. doi: 10.3390/ijms221910238. Int J Mol Sci. 2021. PMID: 34638575 Free PMC article. Review.
-
Haemoadsorption in infective endocarditis: a systematic review.Indian J Thorac Cardiovasc Surg. 2024 May;40(Suppl 1):69-77. doi: 10.1007/s12055-024-01701-0. Epub 2024 Feb 20. Indian J Thorac Cardiovasc Surg. 2024. PMID: 38827548 Free PMC article. Review.
Cited by
-
The Austrian ICU survey : A questionnaire-based evaluation of intensive care medicine in Austria.Wien Klin Wochenschr. 2022 May;134(9-10):351-360. doi: 10.1007/s00508-021-02002-x. Epub 2022 Jan 27. Wien Klin Wochenschr. 2022. PMID: 35084589 Free PMC article.
-
The Potential Role of Extracorporeal Cytokine Removal in Hemodynamic Stabilization in Hyperinflammatory Shock.Biomedicines. 2021 Jul 1;9(7):768. doi: 10.3390/biomedicines9070768. Biomedicines. 2021. PMID: 34356830 Free PMC article. Review.
-
Hemoadsorption in the Management of Septic Shock: A Systematic Review and Meta-Analysis.J Clin Med. 2025 Mar 27;14(7):2285. doi: 10.3390/jcm14072285. J Clin Med. 2025. PMID: 40217734 Free PMC article. Review.
-
Proteomic changes to immune and inflammatory processes underlie lung preservation using ex vivo cytokine adsorption.Front Cardiovasc Med. 2023 Oct 2;10:1274444. doi: 10.3389/fcvm.2023.1274444. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37849943 Free PMC article.
-
Can the cytokine adsorber CytoSorb® help to mitigate cytokine storm and reduce mortality in critically ill patients? A propensity score matching analysis.Ann Intensive Care. 2021 Jul 22;11(1):115. doi: 10.1186/s13613-021-00905-6. Ann Intensive Care. 2021. PMID: 34292421 Free PMC article.
References
-
- https://cytosorb-therapy.com/en/the-therapy/therapeutic-effects/. Accessed 01 Jan 2020.
Associated data
LinkOut - more resources
Full Text Sources
Medical
