

Pre- and postsurgical medical therapy for endometriosis surgery
- PMID: 33206374
- PMCID: PMC8127059
- DOI: 10.1002/14651858.CD003678.pub3
Pre- and postsurgical medical therapy for endometriosis surgery
Abstract
Background: Endometriosis is a common gynaecological condition affecting 10% to 15% of reproductive-age women and may cause dyspareunia, dysmenorrhoea, and infertility. One treatment strategy is combining surgery and medical therapy to reduce the recurrence of endometriosis. Though the combination of surgery and medical therapy appears to be beneficial, there is a lack of clarity about the appropriate timing of when medical therapy should be used in relation with surgery, that is, before, after, or both before and after surgery, to maximize treatment response.
Objectives: To determine the effectiveness of medical therapies for hormonal suppression before, after, or both before and after surgery for endometriosis for improving painful symptoms, reducing disease recurrence, and increasing pregnancy rates.
Search methods: We searched the Cochrane Gynaecology and Fertility (CGF) Group trials register, CENTRAL, MEDLINE, Embase, PsycINFO, CINAHL, and two trials registers in November 2019 together with reference checking and contact with study authors and experts in the field to identify additional studies.
Selection criteria: We included randomized controlled trials (RCTs) which compared medical therapies for hormonal suppression before, after, or before and after, therapeutic surgery for endometriosis.
Data collection and analysis: Two review authors independently extracted data and assessed risk of bias. Where possible, we combined data using risk ratio (RR), standardized mean difference or mean difference (MD) and 95% confidence intervals (CI). Primary outcomes were: painful symptoms of endometriosis as measured by a visual analogue scale (VAS) of pain, other validated scales or dichotomous outcomes; and recurrence of disease as evidenced by EEC (Endoscopic Endometriosis Classification), rAFS (revised American Fertility Society), or rASRM (revised American Society for Reproductive Medicine) scores at second-look laparoscopy.
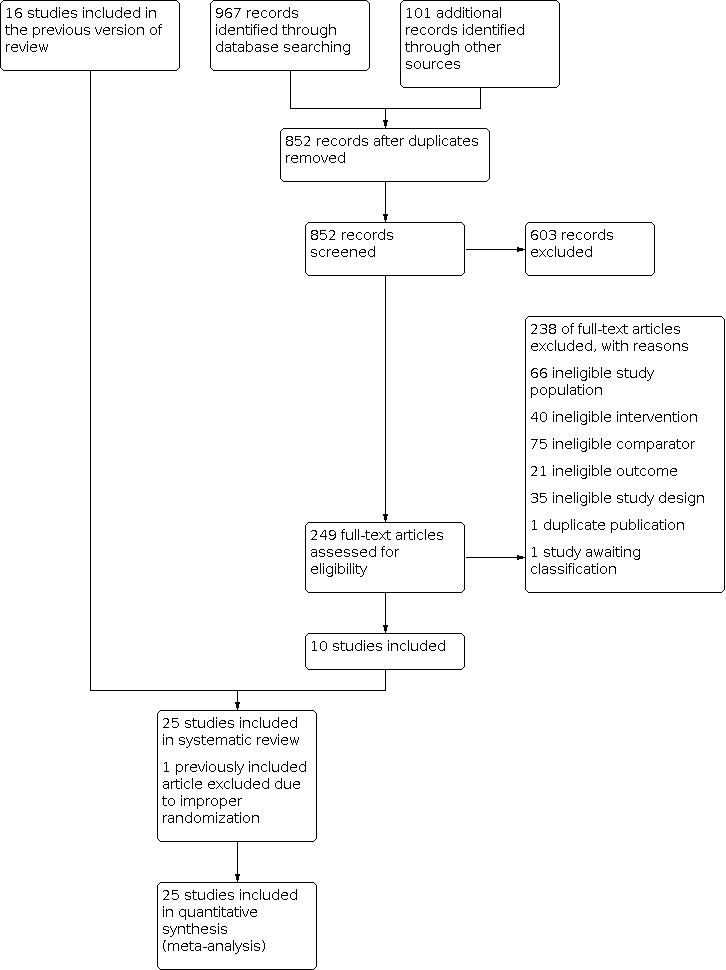
Main results: We included 26 trials with 3457 women with endometriosis. We used the term "surgery alone" to refer to placebo or no medical therapy. Presurgical medical therapy compared with placebo or no medical therapy Compared to surgery alone, we are uncertain if presurgical medical hormonal suppression reduces pain recurrence at 12 months or less (dichotomous) (RR 1.10, 95% CI 0.72 to 1.66; 1 RCT, n = 262; very low-quality evidence) or whether it reduces disease recurrence at 12 months - total (AFS score) (MD -9.6, 95% CI -11.42 to -7.78; 1 RCT, n = 80; very low-quality evidence). We are uncertain if presurgical medical hormonal suppression decreases disease recurrence at 12 months or less (EEC stage) compared to surgery alone (RR 0.88, 95% CI 0.78 to 1.00; 1 RCT, n = 262; very low-quality evidence). We are uncertain if presurgical medical hormonal suppression improves pregnancy rates compared to surgery alone (RR 1.16, 95% CI 0.99 to 1.36; 1 RCT, n = 262; very low-quality evidence). No trials reported pelvic pain at 12 months or less (continuous) or disease recurrence at 12 months or less. Postsurgical medical therapy compared with placebo or no medical therapy We are uncertain about the improvement observed in pelvic pain at 12 months or less (continuous) between postsurgical medical hormonal suppression and surgery alone (MD -0.48, 95% CI -0.64 to -0.31; 4 RCTs, n = 419; I2 = 94%; very low-quality evidence). We are uncertain if there is a difference in pain recurrence at 12 months or less (dichotomous) between postsurgical medical hormonal suppression and surgery alone (RR 0.85, 95% CI 0.65 to 1.12; 5 RCTs, n = 634; I2 = 20%; low-quality evidence). We are uncertain if postsurgical medical hormonal suppression improves disease recurrence at 12 months - total (AFS score) compared to surgery alone (MD -2.29, 95% CI -4.01 to -0.57; 1 RCT, n = 51; very low-quality evidence). Disease recurrence at 12 months or less may be reduced with postsurgical medical hormonal suppression compared to surgery alone (RR 0.30, 95% CI 0.17 to 0.54; 4 RCTs, n = 433; I2 = 58%; low-quality evidence). We are uncertain about the reduction observed in disease recurrence at 12 months or less (EEC stage) between postsurgical medical hormonal suppression and surgery alone (RR 0.80, 95% CI 0.70 to 0.91; 1 RCT, n = 285; very low-quality evidence). Pregnancy rate is probably increased with postsurgical medical hormonal suppression compared to surgery alone (RR 1.22, 95% CI 1.06 to 1.39; 11 RCTs, n = 932; I2 = 24%; moderate-quality evidence). Pre- and postsurgical medical therapy compared with surgery alone or surgery and placebo There were no trials identified in the search for this comparison. Presurgical medical therapy compared with postsurgical medical therapy We are uncertain about the difference in pain recurrence at 12 months or less (dichotomous) between postsurgical and presurgical medical hormonal suppression therapy (RR 1.40, 95% CI 0.95 to 2.07; 2 RCTs, n = 326; I2 = 2%; low-quality evidence). We are uncertain about the difference in disease recurrence at 12 months or less (EEC stage) between postsurgical and presurgical medical hormonal suppression therapy (RR 1.10, 95% CI 0.95 to 1.28; 1 RCT, n = 273; very low-quality evidence). We are uncertain about the difference in pregnancy rate between postsurgical and presurgical medical hormonal suppression therapy (RR 1.05, 95% CI 0.91 to 1.21; 1 RCT, n = 273; very low-quality evidence). No trials reported pelvic pain at 12 months or less (continuous), disease recurrence at 12 months - total (AFS score) or disease recurrence at 12 months or less (dichotomous). Postsurgical medical therapy compared with pre- and postsurgical medical therapy There were no trials identified in the search for this comparison. Serious adverse effects for medical therapies reviewed There was insufficient evidence to reach a conclusion regarding serious adverse effects, as no studies reported data suitable for analysis.
Authors' conclusions: Our results indicate that the data about the efficacy of medical therapy for endometriosis are inconclusive, related to the timing of hormonal suppression therapy relative to surgery for endometriosis. In our various comparisons of the timing of hormonal suppression therapy, women who receive postsurgical medical therapy compared with no medical therapy or placebo may experience benefit in terms of disease recurrence and pregnancy. There is insufficient evidence regarding hormonal suppression therapy at other time points in relation to surgery for women with endometriosis.
Copyright © 2020 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
IC: none.
VV: none.
AC: none.
AM: participated in speaker bureau and/or advisory boards for Allergan, Abbvie, Bayer, Hologic, Medtronic, Pfizer, Baxter
AZ: received honoraria for educational presentations outside the submitted work.
AB: Dr. Black has received a honorarium for participating as a consultant on advisory boards, presenting at continuing medical education events, and developing patient and health care provider educational tools from the following companies: Pfizer, Merck, Bayer.
CA: none.
JM: none.
Figures














Update of
-
Pre and post operative medical therapy for endometriosis surgery.Cochrane Database Syst Rev. 2004;2004(3):CD003678. doi: 10.1002/14651858.CD003678.pub2. Cochrane Database Syst Rev. 2004. Update in: Cochrane Database Syst Rev. 2020 Nov 18;11:CD003678. doi: 10.1002/14651858.CD003678.pub3. PMID: 15266496 Free PMC article. Updated.
References
References to studies included in this review
Alkatout 2013 {published data only}
-
- Alkatout I, Mettler L, Beteta C, Hedderich J, Jonat W, Schollmeyer T, et al. Combined surgical and hormone therapy for endometriosis is the most effective treatment: prospective, randomized, controlled trial. Journal of Minimally Invasive Gynaecology 2013;20(4):473-81. - PubMed
Angioni 2015 {published data only}
-
- Angioni S, Pontis A, Dessole M, Surico D, De Cicco Nardone C, Melis I. Pain control and quality of life after laparoscopic en-block resection of deep infiltrating endometriosis (DIE) vs. incomplete surgical treatment with or without GnRHa administration after surgery. Archives of Gynecology and Obstetrics 2015;291:363-70. - PubMed
Audebert 1998 {published data only}
-
- Audebert A, Descamps P, Marret H, Ory-Lavollee L, Bailleul F, Hamamah S. Pre or post-operative medical treatment with nafarelin in stage III–IV endometriosis: a French multicenter study. Obstetrics and Gynecology 1998;79:145-8. - PubMed
Bianchi 1999 {published data only}
-
- Bianchi S, Busacca M, Agnoli B, Candiani M, Calia C, Vignali M. Effects of 3 month therapy with danazol after laparoscopic surgery for stage III/IV endometriosis: a randomized study. Human Reproduction 1999;14(5):1335-7. - PubMed
Busacca 2001 {published data only}
-
- Busacca M, Somigliana E, Bianchi S, Marinis SD, Calia C, Candiani M, et al. Post-operative GnRH analogue treatment after conservative surgery for symptomatic endometriosis stage III–IV: a randomized controlled trial. Human Reproduction 2001;16(11):2399-402. - PubMed
Cucinella 2013 {published data only}
-
- Cucinella G, Granese R, Calagna G, Svelato A, Saitta S, Tonni G, et al. Oral contraceptives in the prevention of endometrioma recurrence: does the different progestins used make a difference? Archives of Gynecology and Obstetrics 2013;288:821-7. - PubMed
Donnez 1994 {published data only}
-
- Donnez J, Anaf V, Nisolle M, Clerckx-Braun F, Gillerot S, Casanas-Roux F. Ovarian endometrial cysts: the role of gonadotropin-releasing hormone agonist and/or drainage. Fertility and Sterility 1994;62(1):63-6. - PubMed
Hornstein 1997 {published data only}
-
- Hornstein MD, Hemmings R, Yuzpe AA, Heinrichs WL. Use of nafarelin versus placebo after reductive laparoscopic surgery for endometriosis. Fertility and Sterility 1997;68(5):860-4. - PubMed
Huang 2018 {published data only}
-
- Huang C, Wu M, Liu Z, Shi H, Han Y, Song X. Clinical efficacy and safety of gonadotropin-releasing hormone agonist combined with laparoscopic surgery in the treatment of endometriosis. International Journal of Clinical and Experimental Medicine 2018;11:4132-7.
Loverro 2001 {published data only}
-
- Loverro G, Santillo V, Pansini MV, Lorusso F, Depalo R, Selvaggi L. Are GnRH agonists helpful in the therapy of endometriosis after surgical treatment? Human Reproduction 2001;16 Suppl(1):96.
Loverro 2008 {published data only}
-
- Loverro G, Carriero C, Rossi AC, Putignano G, Nicolardi V, Selvaggi L. A randomized study comparing triptorelin or expectant management following conservative laparoscopic surgery for symptomatic stage III–IV endometriosis. European Journal of Obstetrics, Gynecology, and Reproductive Biology 2008;136(2):194-8. - PubMed
Muzii 2000 {published data only}
-
- Muzii L, Marana R, Caruana P, Catalano GF, Margutti F, Panici PB. Postoperative administration of monophasic combined oral contraceptives after laparoscopic treatment of ovarian endometriomas: a prospective, randomized trial. American Journal of Obstetrics and Gynecology 2000;183(3):588-92. - PubMed
Parazzini 1994 {published data only}
-
- Parazzini F, Fedele L, Busacca M, Falsetti L, Pellegrini S, Venturini PL, et al. Postsurgical medical treatment of advanced endometriosis: results of a randomized clinical trial. American Journal of Obstetrics and Gynecology 1994;171:1205-7. - PubMed
Rickes 2002 {published data only}
-
- Rickes D, Nickel I, Kropf S, Kleinstein J. Increased pregnancy rates after ultralong postoperative therapy with gonadotropin-releasing hormone analogs in patients with endometriosis. Fertility and Sterility 2002;78:757-62. - PubMed
Seracchioli 2010a {published data only}
-
- Seracchioli R, Mabrouk M, Frascà C, Manuzzi L, Montanari G, Keramyda A, et al. Long-term cyclic and continuous oral contraceptive therapy and endometrioma recurrence: a randomized controlled trial. Fertility and Sterility 2010;93:52-6. - PubMed
Seracchioli 2010b {published data only}
-
- Seracchioli R, Mabrouk M, Frascà C, Manuzzi L, Savelli L, Venturoli S. Long-term oral contraceptive pills and postoperative pain management after laparoscopic excision of ovarian endometrioma: a randomized controlled trial. Fertility and Sterility 2010;94:464-71. - PubMed
Sesti 2007 {published data only}
-
- Sesti F, Pietropolli A, Capozzolo T, Broccoli P, Pierangeli S, Bollea MR, et al. Hormonal suppression treatment or dietary therapy versus placebo in the control of painful symptoms after conservative surgery for endometriosis stage III-IV. A randomized comparative trial. Fertility and Sterility 2007;88(6):1541-7. - PubMed
Sesti 2009 {published data only}
-
- Sesti F, Capozzolo T, Pietropolli A, Marziali M, Bollea MR, Piccione E. Recurrence rate of endometrioma after laparoscopic cystectomy: a comparative randomized trial between post-operative hormonal suppression treatment or dietary therapy vs. placebo. European Journal of Obstetrics and Gynaecology and Reproductive Biology 2009;147:72-7. - PubMed
Shaw 2001 {published data only}
-
- Shaw R, Garry R, McMillan L, Sutton C, Wood S, Harrison R, et al. A prospective randomized open study comparing goserelin (Zoladex) plus surgery and surgery alone in the management of ovarian endometriomas. Gynaecological Endoscopy 2001;10:151-7.
Tanmahasamut 2017 {published data only}
-
- Tanmahasamut P, Saejong R, Rattanachaiyanont M, Angsuwathana S, Techatraisak K, Sanga-areekul N. Postoperative desogestrel for pelvic endometriosis-related pain: a randomized controlled trial. Gynecological Endocrinology 2017;33:534-9. - PubMed
Telimaa 1987 {published data only}
-
- Telimaa S, Ronnberg L, Kauppila A. Placebo-controlled comparison of danazol and high-dose medroxyprogesterone acetate in the treatment of endometriosis after conservative surgery. Gynecological Endocrinology 1987;1(4):363-71. - PubMed
Tsai 2004 {published data only}
-
- Tsai Y-L, Hwang J-L, Loo T-C, Cheng W-C, Chuang J, Seow K-M. Short-term postoperative GnRH analogue or danazol treatment after conservative surgery for stage III or IV endometriosis before ovarian stimulation: a prospective, randomized study. Journal of Reproductive Medicine 2004;49(12):955-9. - PubMed
Vercellini 1999 {published data only}
-
- Vercellini P, Crosignani PG, Fadini R, Radici E, Belloni C, Sismondi P. A gonadotrophin-releasing hormone agonist compared with expectant management after conservative surgery for symptomatic endometriosis. British Journal of Obstetrics and Gynaecology 1999;106:672-7. - PubMed
Yang 2006 {published data only (unpublished sought but not used)}
-
- Yang D, Ma W, Qu F, MA B. Comparative study on the efficiency of yiweining and gestrinone for post-operational treatment of stage III endometriosis. Chinese Journal of Integrative Medicine 2006;12(3):218-20. - PubMed
Yang 2018 {published data only}
-
- Yang Y, Zhu W, Chen S, Zhang G, Chen M, Zhuang Y. Laparoscopic surgery combined with GnRH agonist in endometriosis. Journal of the College of Physicians and Surgeons Pakistan 2018;29:313-6. - PubMed
References to studies excluded from this review
Batioglu 1997 {published data only}
-
- Batioglu S, Haberai A, Celikkanat H. Comparison of GnRH agonist administration before and after laparoscopic drainage of endometriomas. Journal of Gynecologic Surgery 1997;13(1):17-21.
Morgante 1999 {published data only}
-
- Morgante G, Ditto A, Marca AL, Leo VD. Low-dose danazol after combined surgical and medical therapy reduces the incidence of pelvic pain in women with moderate and severe endometriosis. Human Reproduction 1999;14(9):2371-4. - PubMed
Schindler 1998 {published data only}
-
- Schindler AE, Buhler K, Lubben G, Kienle E. Managment of endometriosis through a combined medical-surgical approach [Was leistet die kombinierte chirurgisch-hormonell Therapie zum Management der Endometriose]. Zentralblatt fur Gynakologie 1998;120:183-90. - PubMed
Shawki 2002 {published data only}
-
- Shawki O, Hamza H, Sattar M. Mild endometriosis, to treat or not treat: randomized controlled trial comparing diagnostic laparoscopy with no further treatment versus post operative Zoladex in cases with infertility associated with stage I, II endometriosis. Fertility and Sterility 2002;77 Suppl 1:13.
Vercellini 2003 {published data only}
-
- Vercellini P, Frontino G, Giorgi OD, Aimi G, Zaina B, Crosignani PG. Comparison of a levonorgestrel-releasing intrauterine device versus expectant management after conservative surgery for symptomatic endometriosis: a pilot study. Fertility and Sterility 2003;80(2):305-9. - PubMed
Ylanen 2003 {published data only}
-
- Ylanen K, Laatikainen T, Lahteenmaki P, Moo-Young AJ. Subdermal progestin implant (Nestorone) in the treatment of endometriosis: clinical response to various doses. Acta Obstetricia et Gynecologica Scandinavica 2003;82:167-72. - PubMed
References to studies awaiting assessment
Roghaei 2010 {published data only}
-
- Roghaei MA, Tehrany HG, Taherian A, Koleini N. Effects of letrozole compared with danazol on patients with confirmed endometriosis: a randomized clinical trial. International Journal of Fertility and Sterility 2010;4:67-72.
Additional references
Acien 2013
ASRM 1997
-
- American Society for Reproductive Medicine. Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertility and Sterility 1997;67(5):817-21. - PubMed
Bazot 2017
-
- Bazot M, Darai E. Diagnosis of deep endometriosis: clinical examination, ultrasonography, magnetic resonance imaging, and other techniques. Fertility and Sterility 2017;108(6):886-94. - PubMed
Bedaiwy 2017
-
- Bedaiwy MA, Allaire C, Alfaraj S. Long-term medical management of endometriosis with dienogest and with a gonadotropin-releasing hormone agonist and add-back hormone therapy. Fertility and Sterility 2017;107(3):537-48. - PubMed
Brown 2014
Covidence [Computer program]
-
- Covidence. Melbourne, Australia: Veritas Health Innovation. Available at covidence.org.
Donnez 1987
-
- Donnez J, Lemaire-Rubbers M, Karaman Y, Nisolle-Pochet M, Casanas-Roux F. Combined (hormonal and microsurgical) therapy in infertile women with endometriosis. Fertility and Sterility 1987;48(2):239-42. - PubMed
Donnez 2004
-
- Donnez J, Pirard C, Smets M, Jadoul P, Squifflet J. Surgical management of endometriosis. Best Practice & Research: Clinical Obstetrics & Gynaecology 2004;18(2):329-48. - PubMed
Duffy 2020
-
- Duffy JMN, Hirsch M, Vercoe M, Abbott J, Barker C, Collura B, et al. A core outcome set for future endometriosis research: an international consensus development study. BJOG: An International Journal of Obstetrics & Gynaecology 2020;127:967– 974. - PubMed
Dunselman 2014
-
- Dunselman GA, Vermeulen N, Becker C, Calhaz-Jorge C, D'Hooghe T, De Bie B, et al. ESHRE guideline: management of women with endometriosis. Human Reproduction 2014;3:400-12. - PubMed
GRADEpro GDT [Computer program]
-
- GRADEpro GDT. Hamilton (ON): McMaster University (developed by Evidence Prime). Available at gradepro.org.
Hemmings 1998
-
- Hemmings R. Combined treatment of endometriosis, GnRH agonists and laparoscopic surgery. Journal of Reproductive Medicine 1998;43 Suppl(2):316-20. - PubMed
Higgins 2009
-
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Intervention. Chichester (UK): John Wiley & Sons, 2009.
Higgins 2011
-
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Johnson 2017
-
- Johnson NP, Hummelshoj L, Adamson GD, Keckstein J, Taylor HS, Abrao Mauricio S, et al. World endometriosis society consensus on the classification of endometriosis. Human Reproduction 2017;32(2):315-24. - PubMed
Kettel 1989
-
- Kettel LM, Murphy AA. Combination medical and surgical therapy for infertile patients with endometriosis. Obstetrics and Gynecology Clinics of North America 1989;16(1):167-77. - PubMed
Koninckx 2019
-
- Koninckx PR, Ussia A Adamyan L, Wattiez A, Gomel V, Martin DC. Pathogenesis of endometriosis: the genetic/epigenetic theory. Fertility and Sterility 2019;111(2):327-40. - PubMed
Lefebvre 2011
-
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Leyland 2010
-
- Leyland N, Casper R, Laberge P, Singh SS, Allen L, Arendas K, et al. Endometriosis: diagnosis and management. Journal of Obstetrics and Gynaecology Canada 2010;32(7):S1-3. - PubMed
Lv 2009
Macer 2012
Missmer 2003
-
- Missmer SA, Cramer DW. The epidemiology of endometriosis. Obstetrics and Gynecology Clinics of North America 2003;30(1):1-19, vii. - PubMed
Review Manager 2014 [Computer program]
-
- Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Somigliana 2017
-
- Somigliana E, Busnelli A, Benaglia L, Vigana P, Leonardi M, Paffoni A, et al. Postoperative hormonal therapy after surgical excision of deep endometriosis. European Journal of Obstetrics and Gynecology and Reproductive Biology 2017;209:77-80. - PubMed
Stephansson 2009
-
- Stephansson O, Kieler H, Granath F, Falconer H. Endometriosis, assisted reproduction technology, and risk of adverse pregnancy outcome. Human Reproduction 2009;24(9):2341-7. - PubMed
Thomas 1992
-
- Thomas EJ. Combining medical and surgical treatment for endometriosis: the best of both worlds? British Journal of Obstetrics and Gynaecology 1992;99 Suppl 7:5-8. - PubMed
Vercellini 2013
-
- Vercellini P, Matteis SD, Somigliana E, Buggio L, Frattaruolo MP, Fedele L. Long-term adjuvant therapy for the prevention of postoperative endometrioma recurrence: a systematic review and meta-analysis. Acta Obstetricia et Gynecologica Scandinavica 2013;92(1):8-16. - PubMed
Vercellini 2014
-
- Vercellini P, Vigano P, Somigliana E, Fedele L. Endometriosis: pathogenesis and treatment. National Review of Endocrinology 2014;10:261-75. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical