

Randomized Phase II Trial of Anthracycline-free and Anthracycline-containing Neoadjuvant Carboplatin Chemotherapy Regimens in Stage I-III Triple-negative Breast Cancer (NeoSTOP)
- PMID: 33208340
- PMCID: PMC7887017
- DOI: 10.1158/1078-0432.CCR-20-3646
Randomized Phase II Trial of Anthracycline-free and Anthracycline-containing Neoadjuvant Carboplatin Chemotherapy Regimens in Stage I-III Triple-negative Breast Cancer (NeoSTOP)
Abstract
Purpose: Addition of carboplatin (Cb) to anthracycline chemotherapy improves pathologic complete response (pCR), and carboplatin plus taxane regimens also yield encouraging pCR rates in triple-negative breast cancer (TNBC). Aim of the NeoSTOP multisite randomized phase II trial was to assess efficacy of anthracycline-free and anthracycline-containing neoadjuvant carboplatin regimens.
Patients and methods: Patients aged ≥18 years with stage I-III TNBC were randomized (1:1) to receive either paclitaxel (P) weekly × 12 plus carboplatin AUC6 every 21 days × 4 followed by doxorubicin/cyclophosphamide (AC) every 14 days × 4 (CbP → AC, arm A), or carboplatin AUC6 + docetaxel (D) every 21 days × 6 (CbD, arm B). Stromal tumor-infiltrating lymphocytes (sTIL) were assessed. Primary endpoint was pCR in breast and axilla. Other endpoints included residual cancer burden (RCB), toxicity, cost, and event-free (EFS) and overall survival (OS).
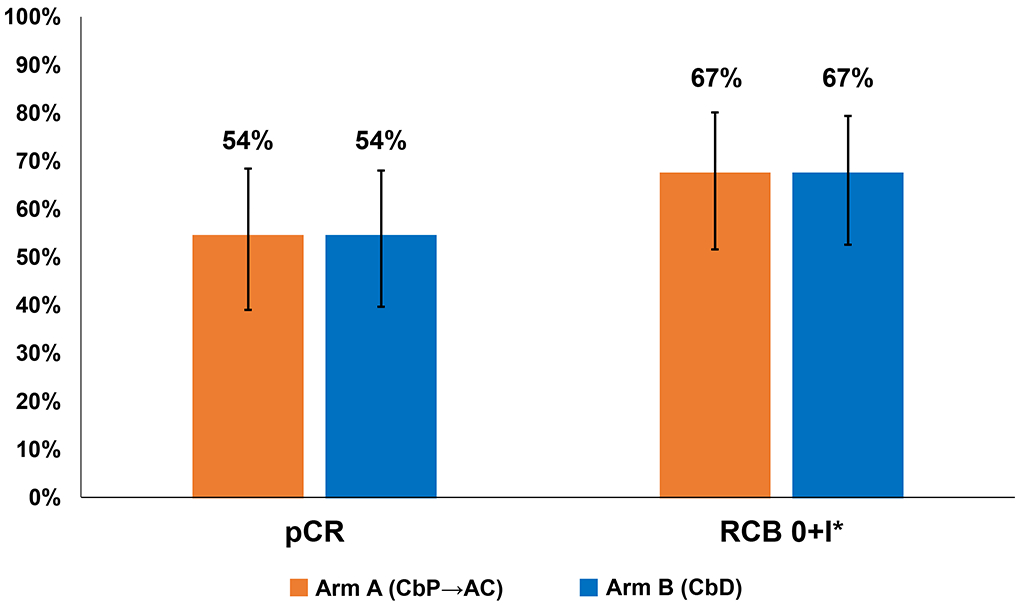
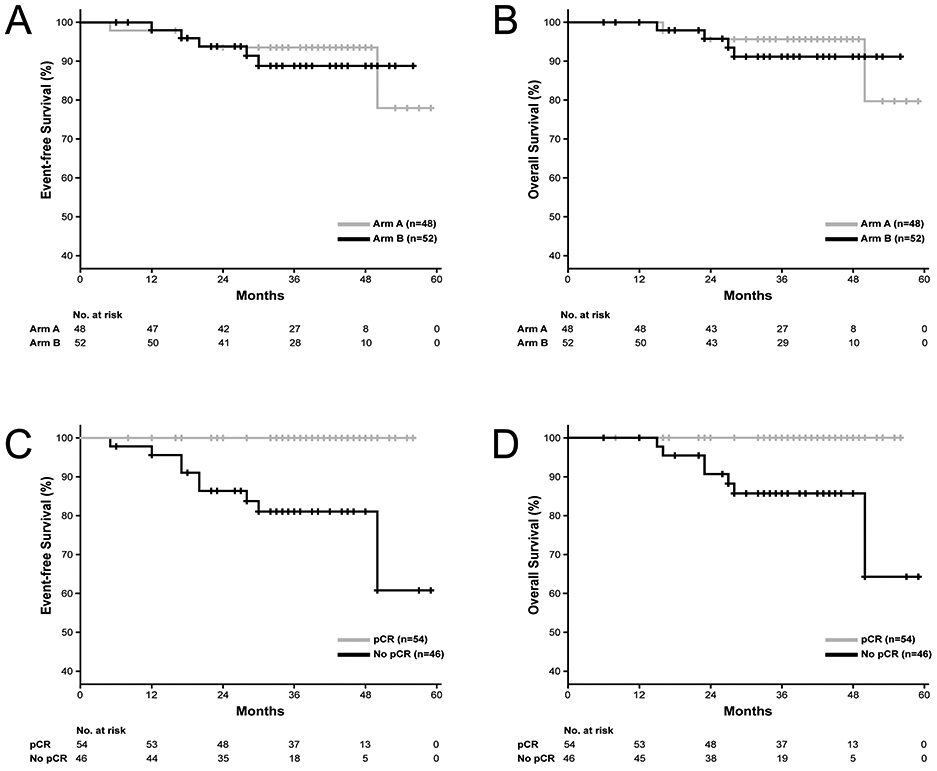
Results: One hundred patients were randomized; arm A (n = 48) or arm B (n = 52). pCR was 54% [95% confidence interval (CI), 40%-69%] in arm A and 54% (95% CI, 40%-68%) in arm B. RCB 0+I rate was 67% in both arms. Median sTIL density was numerically higher in those with pCR compared with those with residual disease (20% vs. 5%; P = 0.25). At median follow-up of 38 months, EFS and OS were similar in the two arms. Grade 3/4 adverse events were more common in arm A compared with arm B, with the most notable differences in neutropenia (60% vs. 8%; P < 0.001) and febrile neutropenia (19% vs. 0%; P < 0.001). There was one treatment-related death (arm A) due to acute leukemia. Mean treatment cost was lower for arm B compared with arm A (P = 0.02).
Conclusions: The two-drug CbD regimen yielded pCR, RCB 0+I, and survival rates similar to the four-drug regimen of CbP → AC, but with a more favorable toxicity profile and lower treatment-associated cost.
©2020 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Liedtke C, Mazouni C, Hess KR, Andre F, Tordai A, Mejia JA, et al. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J Clin Oncol. 2008;26(8):1275–81. - PubMed
-
- Dent R, Trudeau M, Pritchard KI, Hanna WM, Kahn HK, Sawka CA, et al. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res. 2007;13(15 Pt 1):4429–34. - PubMed
-
- National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: breast cancer2019 May 23, 2019. Available from: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf.
-
- Burstein HJ, Curigliano G, Loibl S, Dubsky P, Gnant M, Poortmans P, et al. Estimating the benefits of therapy for early-stage breast cancer: the St. Gallen International Consensus Guidelines for the primary therapy of early breast cancer 2019. Ann Oncol. 2019;30(10):1541–57. - PubMed
-
- Cortazar P, Geyer CE. Pathological complete response in neoadjuvant treatment of breast cancer. Ann Surg Oncol. 2015;22(5):1441–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
