

Identification of a Synthetic Lethal Relationship between Nucleotide Excision Repair Deficiency and Irofulven Sensitivity in Urothelial Cancer
- PMID: 33208343
- PMCID: PMC8026514
- DOI: 10.1158/1078-0432.CCR-20-3316
Identification of a Synthetic Lethal Relationship between Nucleotide Excision Repair Deficiency and Irofulven Sensitivity in Urothelial Cancer
Abstract
Purpose: Cisplatin-based chemotherapy is a first-line treatment for muscle-invasive and metastatic urothelial cancer. Approximately 10% of bladder urothelial tumors have a somatic missense mutation in the nucleotide excision repair (NER) gene, ERCC2, which confers increased sensitivity to cisplatin-based chemotherapy. However, a significant subset of patients is ineligible to receive cisplatin-based therapy due to medical contraindications, and no NER-targeted approaches are available for platinum-ineligible or platinum-refractory ERCC2-mutant cases.
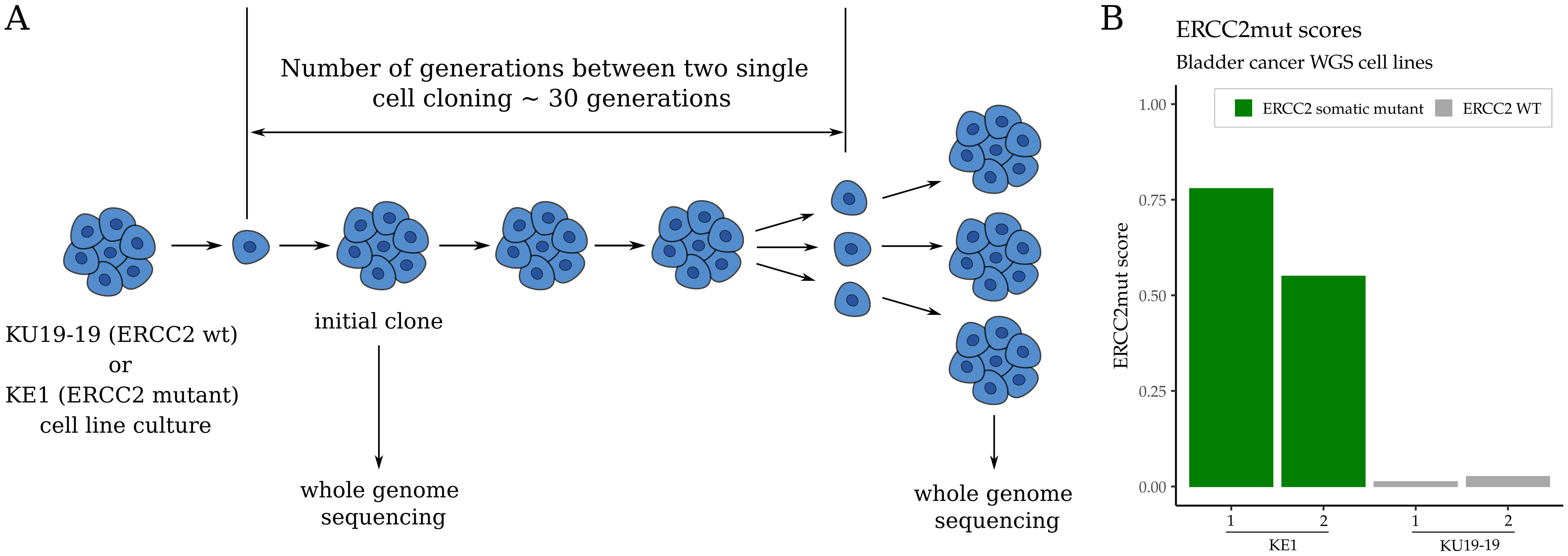
Experimental design: We used a series of NER-proficient and NER-deficient preclinical tumor models to test sensitivity to irofulven, an abandoned anticancer agent. In addition, we used available clinical and sequencing data from multiple urothelial tumor cohorts to develop and validate a composite mutational signature of ERCC2 deficiency and cisplatin sensitivity.
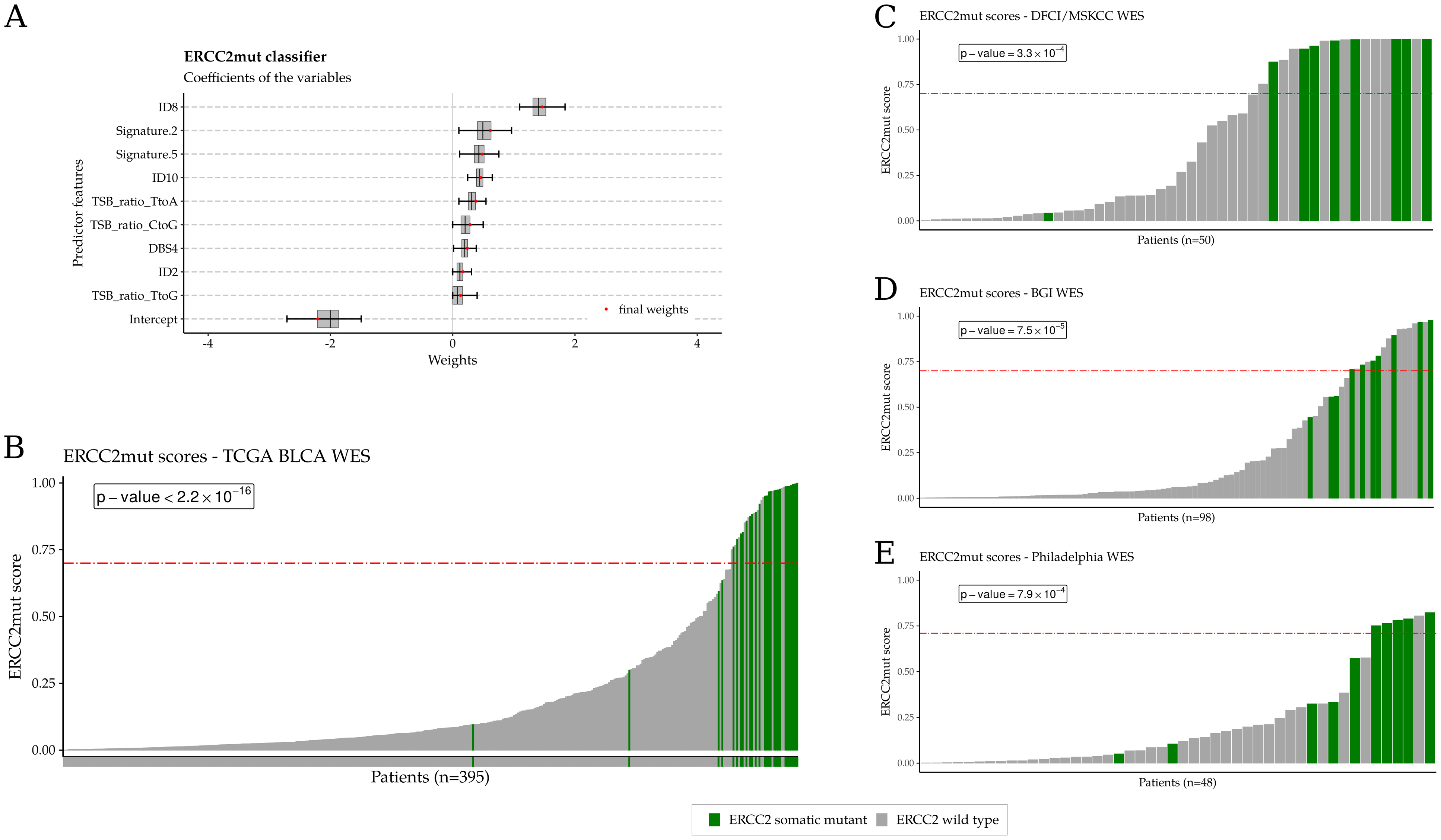
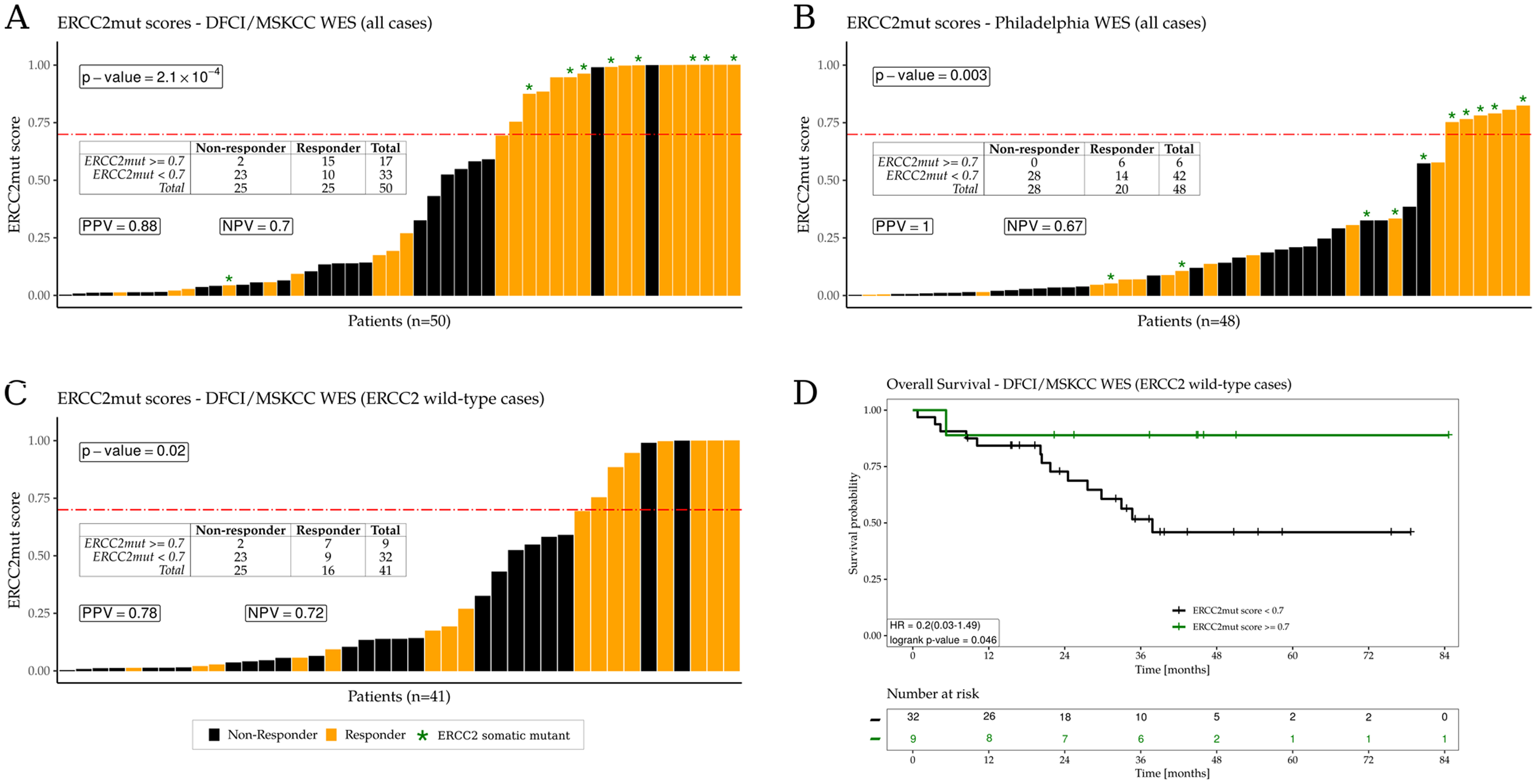
Results: We identified a novel synthetic lethal relationship between tumor NER deficiency and sensitivity to irofulven. Irofulven specifically targets cells with inactivation of the transcription-coupled NER (TC-NER) pathway and leads to robust responses in vitro and in vivo, including in models with acquired cisplatin resistance, while having minimal effect on cells with intact NER. We also found that a composite mutational signature of ERCC2 deficiency was strongly associated with cisplatin response in patients and was also associated with cisplatin and irofulven sensitivity in preclinical models.
Conclusions: Tumor NER deficiency confers sensitivity to irofulven, a previously abandoned anticancer agent, with minimal activity in NER-proficient cells. A composite mutational signature of NER deficiency may be useful in identifying patients likely to respond to NER-targeting agents, including cisplatin and irofulven.See related commentary by Jiang and Greenberg, p. 1833.
©2020 American Association for Cancer Research.
Conflict of interest statement
Conflict of interest
J. Börcsök, M. Diossy, Z. Sztupinszki, K.W. Mouw and Z. Szallasi are listed as co-inventors on a provisional patent owned by Children’s Hospital Boston to quantify the
Figures


Comment on
-
Morning for Irofulven, What Could be fiNER?Clin Cancer Res. 2021 Apr 1;27(7):1833-1835. doi: 10.1158/1078-0432.CCR-20-4708. Epub 2021 Jan 20. Clin Cancer Res. 2021. PMID: 33472911 Free PMC article.
References
-
- Konstantinopoulos PA, Matulonis UA. PARP Inhibitors in Ovarian Cancer: A Trailblazing and Transformative Journey. Clin Cancer Res. 2018;24:4062–5. - PubMed
-
- Marteijn JA, Lans H, Vermeulen W, Hoeijmakers JHJ. Understanding nucleotide excision repair and its roles in cancer and ageing. Nat Rev Mol Cell Biol. 2014;15:465–81. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
