

Gut Microbiota Predict Enterococcus Expansion but Not Vancomycin-Resistant Enterococcus Acquisition
- PMID: 33208515
- PMCID: PMC7677005
- DOI: 10.1128/mSphere.00537-20
Gut Microbiota Predict Enterococcus Expansion but Not Vancomycin-Resistant Enterococcus Acquisition
Abstract
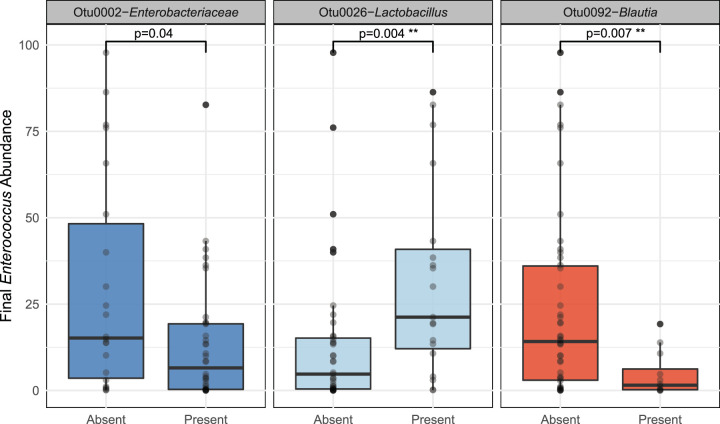
Vancomycin-resistant Enterococcus (VRE) is a leading cause of hospital-acquired infections and continues to spread despite widespread implementation of pathogen-targeted control guidelines. Commensal gut microbiota provide colonization resistance to VRE, but the role of gut microbiota in VRE acquisition in at-risk patients is unknown. To address this gap in our understanding, we performed a case-control study of gut microbiota in hospitalized patients who did (cases) and did not (controls) acquire VRE. We matched case subjects to control subjects by known risk factors and "time at risk," defined as the time elapsed between admission until positive VRE screen. We characterized gut bacterial communities using 16S rRNA gene amplicon sequencing of rectal swab specimens. We analyzed 236 samples from 59 matched case-control pairs. At baseline, case and control subjects did not differ in gut microbiota when measured by community diversity (P = 0.33) or composition (P = 0.30). After hospitalization, gut communities of cases and controls differed only in the abundance of the Enterococcus-containing operational taxonomic unit (OTU), with the gut microbiota of case subjects having more of this OTU than time-matched control subjects (P = 0.01). Otherwise, case and control communities after the time at risk did not differ in diversity (P = 0.33) or community structure (P = 0.12). Among patients who became VRE colonized, those having the Blautia-containing OTU on admission had lower Enterococcus relative abundance once colonized (P = 0.004). Our results demonstrate that the 16S profile of the gut microbiome does not predict VRE acquisition in hospitalized patients, likely due to rapid and profound microbiota change. The gut microbiome does not predict VRE acquisition, but it may be associated with Enterococcus expansion, suggesting that these should be considered two distinct processes.IMPORTANCE The Centers for Disease Control and Prevention estimates that VRE causes an estimated 54,000 infections and 539 million dollars in attributable health care costs annually. Despite improvements in hand washing, environmental cleaning, and antibiotic use, VRE is still prevalent in many hospitals. There is a pressing need to better understand the processes by which patients acquire VRE. Multiple lines of evidence suggest that intestinal microbiota may help some patients resist VRE acquisition. In this large case-control study, we compared the 16S profile of intestinal microbiota on admission in patients that did and did not subsequently acquire VRE. The 16S profile did not predict subsequent VRE acquisition, in part due to rapid and dramatic change in the gut microbiome following hospitalization. However, Blautia spp. present on admission predicted decreased Enterococcus abundance after VRE acquisition, and Lactobacillus spp. present on admission predicted Enterococcus dominance after VRE acquisition. Thus, VRE acquisition and domination may be distinct processes.
Keywords: colonization resistance; hospital-acquired infection; microbiome; vancomycin-resistant Enterococcus.
Copyright © 2020 Chanderraj et al.
Figures




Similar articles
-
Cooperating Commensals Restore Colonization Resistance to Vancomycin-Resistant Enterococcus faecium.Cell Host Microbe. 2017 May 10;21(5):592-602.e4. doi: 10.1016/j.chom.2017.04.002. Cell Host Microbe. 2017. PMID: 28494240 Free PMC article.
-
Distinct but Spatially Overlapping Intestinal Niches for Vancomycin-Resistant Enterococcus faecium and Carbapenem-Resistant Klebsiella pneumoniae.PLoS Pathog. 2015 Sep 3;11(9):e1005132. doi: 10.1371/journal.ppat.1005132. eCollection 2015 Sep. PLoS Pathog. 2015. PMID: 26334306 Free PMC article.
-
Are There Bad ICU Rooms? Temporal Relationship between Patient and ICU Room Microbiome, and Influence on Vancomycin-Resistant Enterococcus Colonization.mSphere. 2022 Feb 23;7(1):e0100721. doi: 10.1128/msphere.01007-21. Epub 2022 Feb 2. mSphere. 2022. PMID: 35107335 Free PMC article.
-
Resistance in Vancomycin-Resistant Enterococci.Infect Dis Clin North Am. 2020 Dec;34(4):751-771. doi: 10.1016/j.idc.2020.08.004. Infect Dis Clin North Am. 2020. PMID: 33131572 Free PMC article. Review.
-
[Vancomycin resistant enterococci in the Netherlands].Ned Tijdschr Geneeskd. 2004 May 1;148(18):878-82. Ned Tijdschr Geneeskd. 2004. PMID: 15152389 Review. Dutch.
Cited by
-
Promiscuous, persistent and problematic: insights into current enterococcal genomics to guide therapeutic strategy.BMC Microbiol. 2024 Mar 28;24(1):103. doi: 10.1186/s12866-024-03243-2. BMC Microbiol. 2024. PMID: 38539119 Free PMC article. Review.
-
The Gut Microbiome Modulates Body Temperature Both in Sepsis and Health.Am J Respir Crit Care Med. 2023 Apr 15;207(8):1030-1041. doi: 10.1164/rccm.202201-0161OC. Am J Respir Crit Care Med. 2023. PMID: 36378114 Free PMC article.
-
In critically ill patients, anti-anaerobic antibiotics increase risk of adverse clinical outcomes.Eur Respir J. 2023 Feb 9;61(2):2200910. doi: 10.1183/13993003.00910-2022. Print 2023 Feb. Eur Respir J. 2023. PMID: 36229047 Free PMC article.
-
Lacticaseibacillus rhamnosus GG Versus Placebo for Eradication of Vancomycin-Resistant Enterococcus faecium in Intestinal Carriers: A Systematic Review and Meta-Analysis.Microorganisms. 2023 Nov 19;11(11):2804. doi: 10.3390/microorganisms11112804. Microorganisms. 2023. PMID: 38004815 Free PMC article. Review.
-
Seaweed polysaccharide relieves hexavalent chromium-induced gut microbial homeostasis.Front Microbiol. 2023 Jan 16;13:1100988. doi: 10.3389/fmicb.2022.1100988. eCollection 2022. Front Microbiol. 2023. PMID: 36726569 Free PMC article.
References
-
- Centers for Disease Control and Prevention. 2019. Antibiotic resistance threats in the United States, 2019. Antibiotic Resistance Coordination and Strategy Unit, Division of Healthcare Quality Promotion, National Center for Emerging and Zoonotic Infectious Diseases, Centers for Disease Control and Prevention, Atlanta, GA.
-
- Weiner LM, Webb AK, Limbago B, Dudeck MA, Patel J, Kallen AJ, Edwards JR, Sievert DM. 2016. Antimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2011–2014. Infect Control Hosp Epidemiol 37:1288−1301. doi:10.1017/ice.2016.174. - DOI - PMC - PubMed
-
- Zirakzadeh A, Gastineau DA, Mandrekar JN, Burke JP, Johnston PB, Patel R. 2008. Vancomycin-resistant enterococcal colonization appears associated with increased mortality among allogeneic hematopoietic stem cell transplant recipients. Bone Marrow Transplant 41:385–392. doi:10.1038/sj.bmt.1705912. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
