

Association of MRI Brain Injury With Outcome After Pediatric Out-of-Hospital Cardiac Arrest
- PMID: 33208547
- PMCID: PMC7884994
- DOI: 10.1212/WNL.0000000000011217
Association of MRI Brain Injury With Outcome After Pediatric Out-of-Hospital Cardiac Arrest
Abstract
Objective: To determine the association between the extent of diffusion restriction and T2/fluid-attenuated inversion recovery (FLAIR) injury on brain MRI and outcomes after pediatric out-of-hospital cardiac arrest (OHCA).
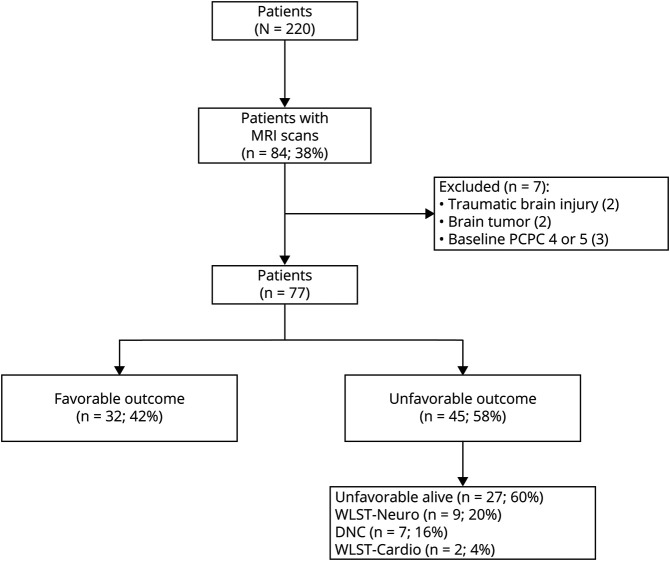
Methods: Diffusion restriction and T2/FLAIR injury were described according to the pediatric MRI modification of the Alberta Stroke Program Early Computed Tomography Score (modsASPECTS) for children from 2005 to 2013 who had an MRI within 14 days of OHCA. The primary outcome was unfavorable neurologic outcome defined as ≥1 change in Pediatric Cerebral Performance Category (PCPC) from baseline resulting in a hospital discharge PCPC score 3, 4, 5, or 6. Patients with unfavorable outcomes were further categorized into alive with PCPC 3-5, dead due to withdrawal of life-sustaining therapies for poor neurologic prognosis (WLST-neuro), or dead by neurologic criteria.
Results: We evaluated MRI scans from 77 patients (median age 2.21 [interquartile range 0.44, 13.07] years) performed 4 (2, 6) days postarrest. Patients with unfavorable outcomes had more extensive diffusion restriction (median 7 [4, 10.3] vs 0 [0, 0] regions, p < 0.001) and T2/FLAIR injury (5.5 [2.3, 8.2] vs 0 [0, 0.75] regions, p < 0.001) compared to patients with favorable outcomes. Area under the receiver operating characteristic curve for the extent of diffusion restriction and unfavorable outcome was 0.96 (95% confidence interval [CI] 0.91, 0.99) and 0.92 (95% CI 0.85, 0.97) for T2/FLAIR injury. There was no difference in extent of diffusion restriction between patients who were alive with an unfavorable outcome and patients who died from WLST-neuro (p = 0.11).
Conclusions: More extensive diffusion restriction and T2/FLAIR injury on the modsASPECTS score within the first 14 days after pediatric cardiac arrest was associated with unfavorable outcomes at hospital discharge.
© 2020 American Academy of Neurology.
Figures




References
-
- Benjamin EJ, Virani SS, Callaway CW, et al. . Heart disease and stroke statistics: 2018 update: a report from the American Heart Association. Circulation 2018;137:e67–e492. - PubMed
-
- Nitta M, Iwami T, Kitamura T, et al. . Age-specific differences in outcomes after out-of-hospital cardiac arrests. Pediatrics 2011;128:e812–e820. - PubMed
-
- Du Pont-Thibodeau G, Fry M, Kirschen M, et al. . Timing and modes of death after pediatric out-of-hospital cardiac arrest resuscitation. Resuscitation 2018;133:160–166. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources