

Light control of RTK activity: from technology development to translational research
- PMID: 33209247
- PMCID: PMC7654314
- DOI: 10.1039/d0sc03570j
Light control of RTK activity: from technology development to translational research
Abstract
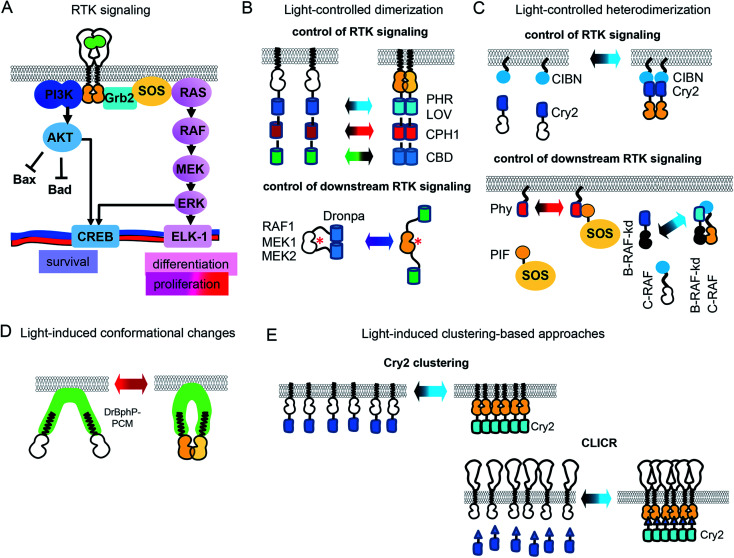
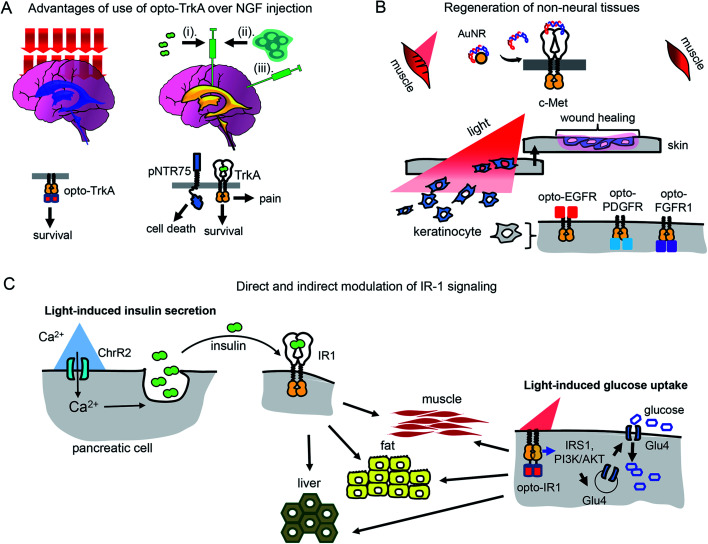
Inhibition of receptor tyrosine kinases (RTKs) by small molecule inhibitors and monoclonal antibodies is used to treat cancer. Conversely, activation of RTKs with their ligands, including growth factors and insulin, is used to treat diabetes and neurodegeneration. However, conventional therapies that rely on injection of RTK inhibitors or activators do not provide spatiotemporal control over RTK signaling, which results in diminished efficiency and side effects. Recently, a number of optogenetic and optochemical approaches have been developed that allow RTK inhibition or activation in cells and in vivo with light. Light irradiation can control RTK signaling non-invasively, in a dosed manner, with high spatio-temporal precision, and without the side effects of conventional treatments. Here we provide an update on the current state of the art of optogenetic and optochemical RTK technologies and the prospects of their use in translational studies and therapy.
This journal is © The Royal Society of Chemistry 2020.
Figures





Similar articles
-
Radiolabelled receptor-tyrosine-kinase targeting drugs for patient stratification and monitoring of therapy response: prospects and pitfalls.Lancet Oncol. 2010 Oct;11(10):992-1000. doi: 10.1016/S1470-2045(10)70088-7. Epub 2010 Jul 26. Lancet Oncol. 2010. PMID: 20667780 Review.
-
Light-activated receptor tyrosine kinases: Designs and applications.Curr Opin Pharmacol. 2022 Apr;63:102197. doi: 10.1016/j.coph.2022.102197. Epub 2022 Mar 1. Curr Opin Pharmacol. 2022. PMID: 35245796 Review.
-
Activation and function of receptor tyrosine kinases in human clear cell renal cell carcinomas.BMC Cancer. 2019 Nov 5;19(1):1044. doi: 10.1186/s12885-019-6159-2. BMC Cancer. 2019. PMID: 31690270 Free PMC article.
-
A Generalizable Optogenetic Strategy to Regulate Receptor Tyrosine Kinases during Vertebrate Embryonic Development.J Mol Biol. 2020 May 1;432(10):3149-3158. doi: 10.1016/j.jmb.2020.03.032. Epub 2020 Apr 8. J Mol Biol. 2020. PMID: 32277988 Free PMC article.
-
Tyrosine kinase receptors as attractive targets of cancer therapy.Crit Rev Oncol Hematol. 2004 Apr;50(1):23-38. doi: 10.1016/j.critrevonc.2003.08.004. Crit Rev Oncol Hematol. 2004. PMID: 15094157 Review.
Cited by
-
Optogenetic Approaches for the Spatiotemporal Control of Signal Transduction Pathways.Int J Mol Sci. 2021 May 18;22(10):5300. doi: 10.3390/ijms22105300. Int J Mol Sci. 2021. PMID: 34069904 Free PMC article. Review.
-
A guide to the optogenetic regulation of endogenous molecules.Nat Methods. 2021 Sep;18(9):1027-1037. doi: 10.1038/s41592-021-01240-1. Epub 2021 Aug 26. Nat Methods. 2021. PMID: 34446923 Review.
-
Optogenetic activation of intracellular signaling based on light-inducible protein-protein homo-interactions.Neural Regen Res. 2022 Jan;17(1):25-30. doi: 10.4103/1673-5374.314293. Neural Regen Res. 2022. PMID: 34100422 Free PMC article.
-
A general approach for engineering RTKs optically controlled with far-red light.Nat Methods. 2022 Jul;19(7):871-880. doi: 10.1038/s41592-022-01517-z. Epub 2022 Jun 9. Nat Methods. 2022. PMID: 35681062
-
Engineering signalling pathways in mammalian cells.Nat Biomed Eng. 2024 Dec;8(12):1523-1539. doi: 10.1038/s41551-024-01237-z. Epub 2024 Sep 5. Nat Biomed Eng. 2024. PMID: 39237709 Free PMC article. Review.
References
-
- Kim H. S., Yoo H. S. Acta Biomater. 2013;9:7371–7380. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources