

Is total arch replacement associated with an increased risk after acute type A dissection?
- PMID: 33209385
- PMCID: PMC7656345
- DOI: 10.21037/jtd-20-871
Is total arch replacement associated with an increased risk after acute type A dissection?
Abstract
Background: The surgical strategy for acute type A aortic dissection (AADA) usually consists of reconstruction of the tear-lesion in the affected part of the ascending aorta. The optimal strategy either to replace the ascending aorta (AAR) or to replace the ascending aorta and the total aortic arch (TAAR) is still under debate. Our study compares the 30-day mortality between AAR and TAAR in AADA surgery.
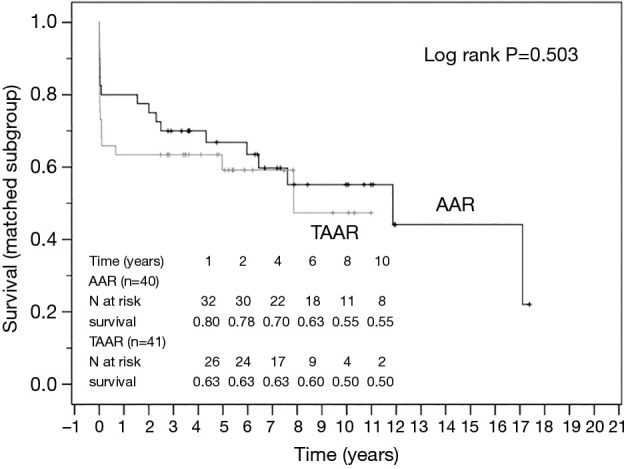
Methods: In this retrospective observational study, we analysed a total patient cohort of 339 patients who underwent surgery for AADA from January 2001 until December 2016. A propensity score-matched analysis between the AAR- and the TAAR-group with 43 patients for each subgroup was subsequently carried out. A multivariable analysis was performed to identify risk-factors for the 30-d-mortality. The 30-day mortality was defined as the primary end-point and long-term survival was the secondary endpoint.
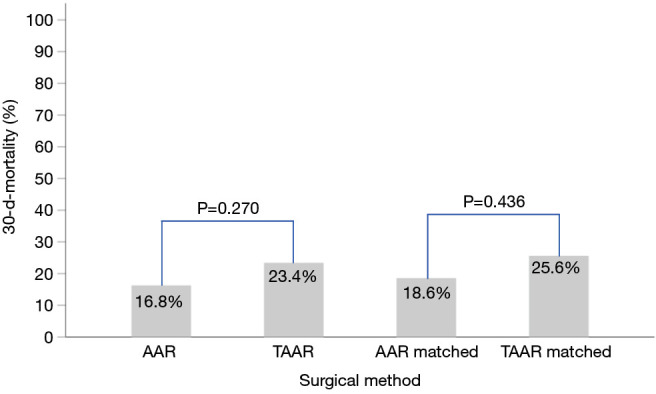
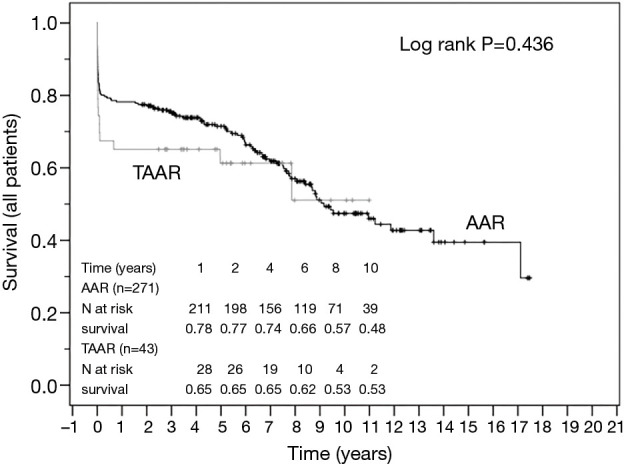
Results: In 292 (86.1%) patients AAR and in 47 (13.9%) patients TAAR was performed for emergent AADA. Patients were older (P=0.049) in the AAR group. The median log Euro-SCORE was 25.5% (12.7; 41.7) for AAR and 19.7% (11.7; 32.2) for the TAAR patient cohort (P=0.12). Operative time, cardiopulmonary bypass- (CPB), cross-clamp- and ischemic time were significantly longer in the TAAR group (P<0.001). The overall 30-day mortality-rate was 17.7% (n=60) but was not significantly different between the two groups (P=0.27). Forty-nine (16.8%) patients died in the AAR and 11 patients (23.4%) in the TAAR group. After propensity-score matching, no difference in mortality was seen between the subgroups as well (P=0.44). Multivariable analysis identified the Euro-SCORE, long operation-time, postoperative dialysis and arrhythmia and administration of red blood cell concentrates as risk factors for 30-day mortality, but not for TAAR versus AAR.
Conclusions: The therapeutic goal in AADA surgery should be the complete restoration of the aorta to avoid further long-term complications and re-operations. Though 30-day mortality and postoperative co-morbidity for AAR are comparable to those in TAAR after treatment of AADA in our analysis, decision-making for the surgical strategy should weigh the operative risk of TAAR against the long-term outcome.
Keywords: Acute type A aortic dissection (AADA); ascending aorta replacement (AAR); total aortic arch replacement (TAAR).
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/jtd-20-871). The authors have no conflicts of interest to declare.
Figures
References
-
- Rampoldi V, Trimarchi S, Eagle KA, Isselbacher Simple risk models to predict surgical mortality in acute type A aortic dissection: The International Registry of Acute Aortic Dissection score. International Registry of Acute Aortic Dissection (IRAD) Investigators. Ann Thorac Surg 2007;83:55-61. 10.1016/j.athoracsur.2006.08.007 - DOI - PubMed
-
- Cecconi M, Lopez E, Zanoli R, Postoperative follow-up of type A aortic dissection experience with 67 patients. G Ital Cardiol 1999;29:898-909. - PubMed
LinkOut - more resources
Full Text Sources