

Prognostic impact of lymph node ratio in patients with pT1-2N1M0 non-small cell lung cancer
- PMID: 33209388
- PMCID: PMC7656357
- DOI: 10.21037/jtd-20-1611
Prognostic impact of lymph node ratio in patients with pT1-2N1M0 non-small cell lung cancer
Abstract
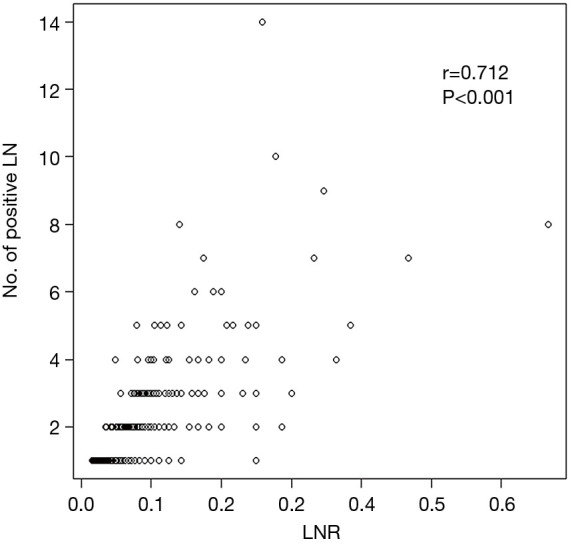
Background: This study evaluated the lymph node ratio (LNR) defined as the ratio of the number of metastatic lymph nodes to the number of dissected lymph nodes as a prognostic factor for survival in patients with pT1-2N1M0 non-small cell lung cancer (NSCLC).
Methods: We retrospectively reviewed 413 patients with pathologic T1-2N1M0 NSCLC after complete surgical resection and mediastinal LN dissection between January 2004 and December 2012. The cut-off value for LNR was determined using χ2 tests, which were calculated using Cox proportional hazards regression model. Based on this model, the optimal cut-off value for LNR was 0.1.
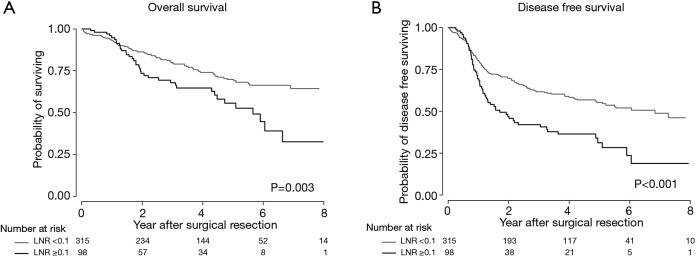
Results: The study included 337 males and 76 females with a mean age of 62 years (range, 34-83 years). Patients with a high LNR (≥0.1) were more likely to be female and have more adenocarcinomas compared with patients with a low LNR (<0.1). The overall survival (OS) and disease-free survival (DFS) rates were significantly worse in the high LNR group than the low LNR group (OS, 55.4% vs. 69.8%, respectively P=0.003; DFS, 33.2% vs. 61.7%, P<0.001). In the multivariate analysis, a high LNR was associated with significantly worse OS [adjusted hazard ratio (aHR), 2.69; 95% confidence interval (CI), 1.74-4.17] and DFS (aHR, 2.41; 95% CI, 1.57-3.68).
Conclusions: LNR is an independent prognostic factor for survival in patients with pT1-2N1M0 NSCLC. These findings may provide useful prognostic information to allow the selection of patients for more aggressive postoperative therapy or follow-up strategies.
Keywords: Lung neoplasm; lymph nodes; non-small cell lung cancer (NSCLC); prognosis; risk factors.
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/jtd-20-1611). The authors have no conflicts of interest to declare.
Figures


References
-
- Liang W, He J, Shen Y, et al. Impact of Examined Lymph Node Count on Precise Staging and Long-Term Survival of Resected Non-Small-Cell Lung Cancer: A Population Study of the US SEER Database and a Chinese Multi-Institutional Registry. J Clin Oncol 2017;35:1162-70. 10.1200/JCO.2016.67.5140 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources