

A systematic review and meta-analysis of thoracoscopic versus thoracotomy sleeve lobectomy
- PMID: 33209400
- PMCID: PMC7656351
- DOI: 10.21037/jtd-20-1855
A systematic review and meta-analysis of thoracoscopic versus thoracotomy sleeve lobectomy
Abstract
Background: Operative safety and oncologic adequacy of thoracoscopic sleeve lobectomy remain controversial. As such, the purpose of this meta-analysis was to evaluate evidence comparing thoracoscopy and thoracotomy in sleeve lobectomy for centrally located non-small cell lung cancer (NSCLC).
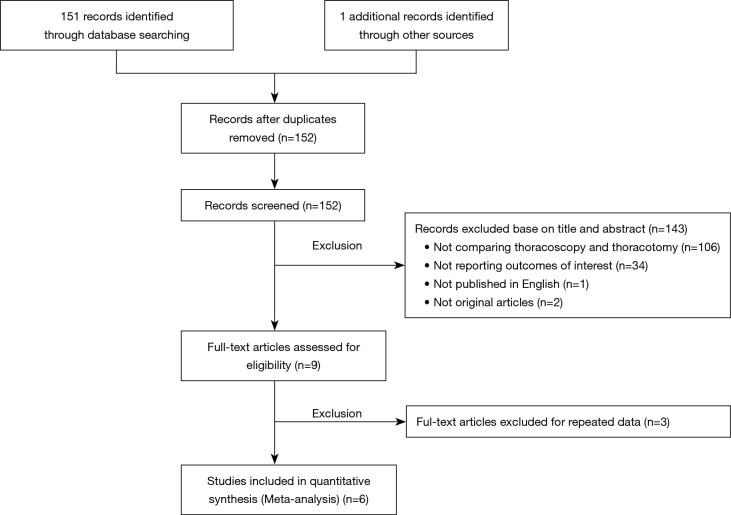
Methods: Electronic searches of PubMed and Web of Science databases were undertaken from inception to March 2020. Comparative studies about thoracoscopic and thoracotomy sleeve lobectomy, with evaluation for perioperative outcomes and oncological results were identified. The following outcomes were measured in this meta-analysis: operating time, blood loss, numbers of lymph node, postoperative hospital stay, chest drainage time, postoperative complication rate, mortality, overall survival (OS). The standardized difference (SMD), relative risk (RR) and hazard ratio (HR) with 95% confidence intervals (CI) were pooled using Stata software.
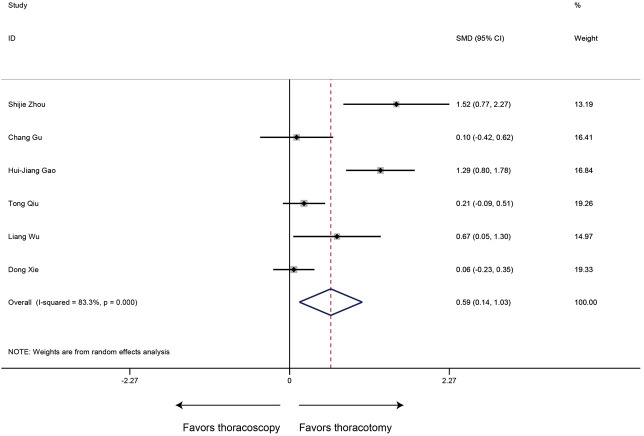
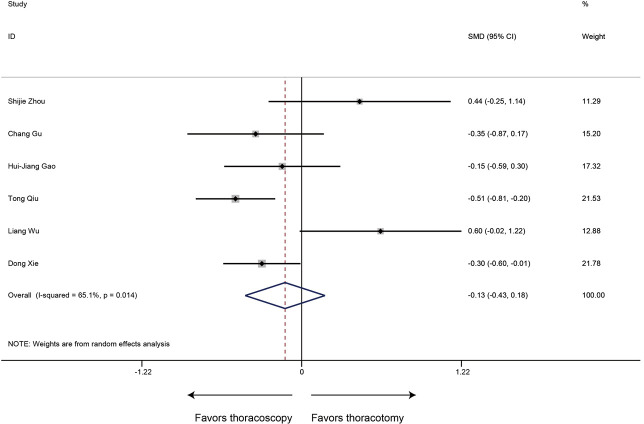
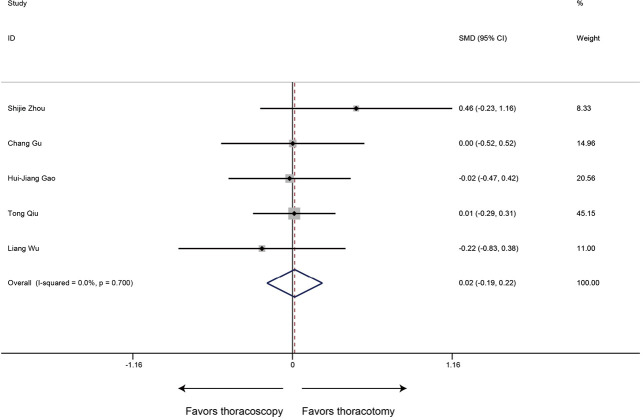
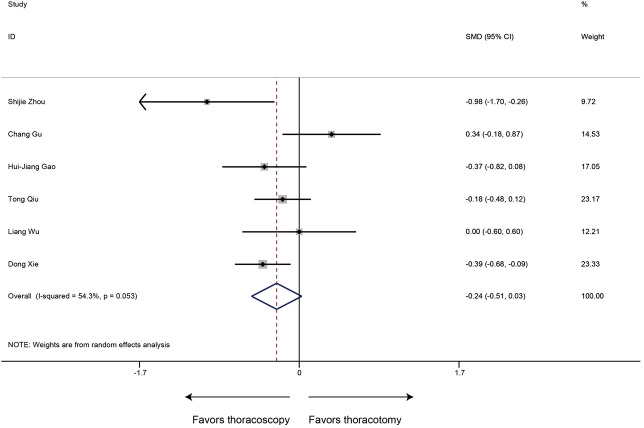
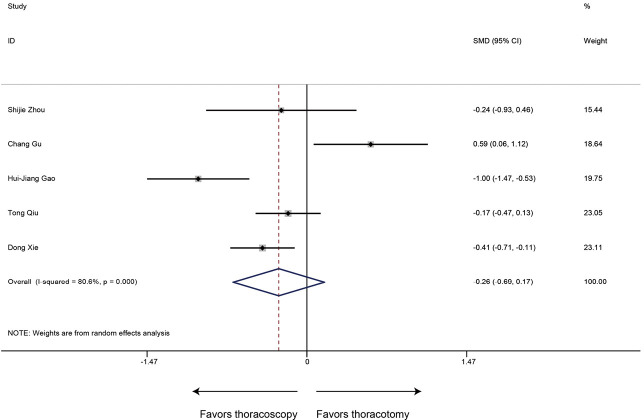
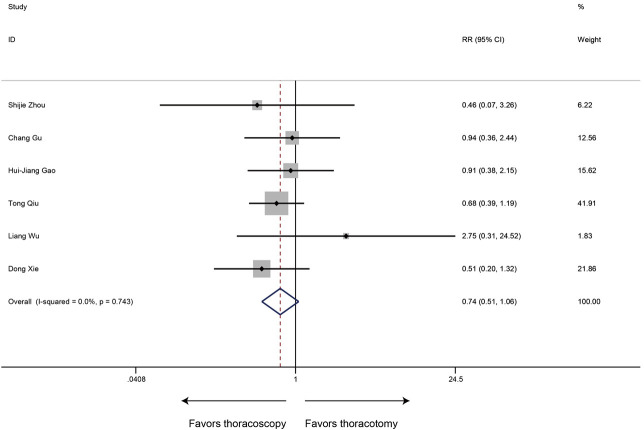
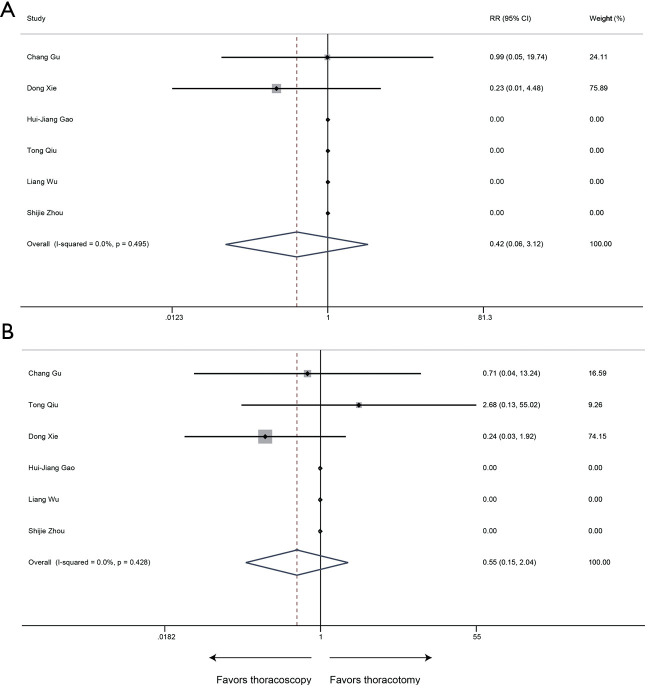
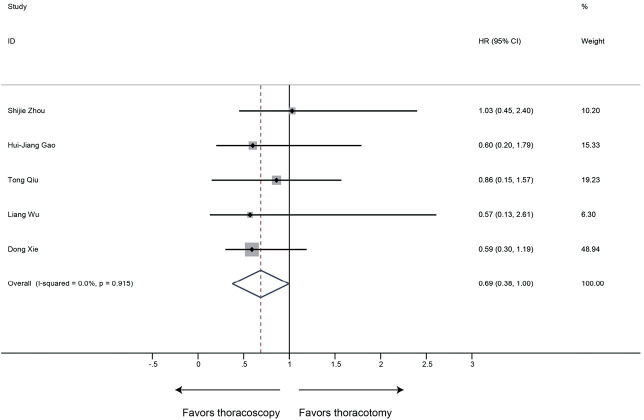
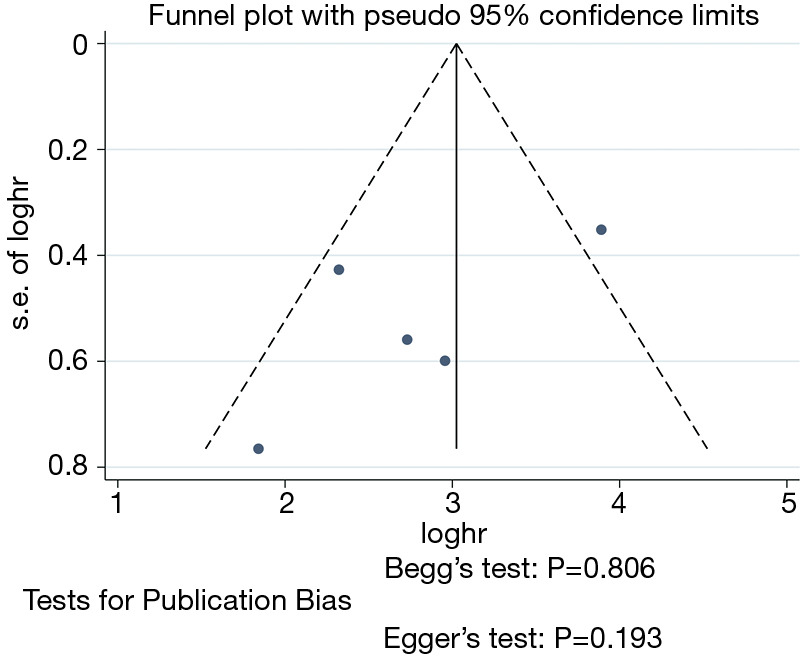
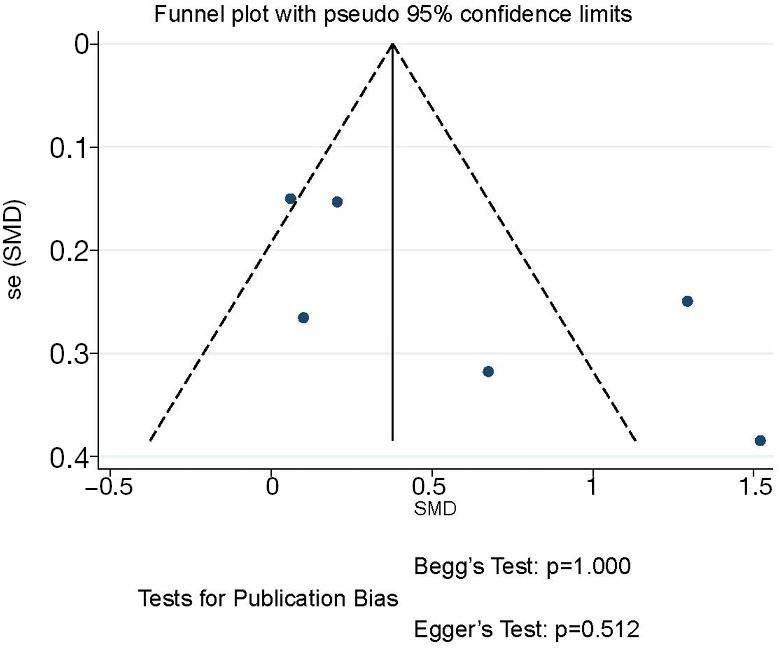
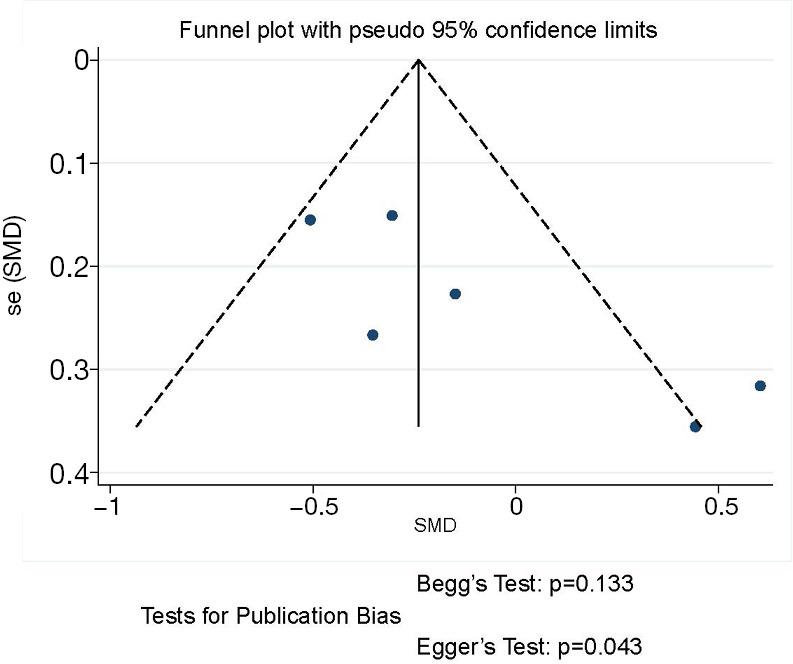
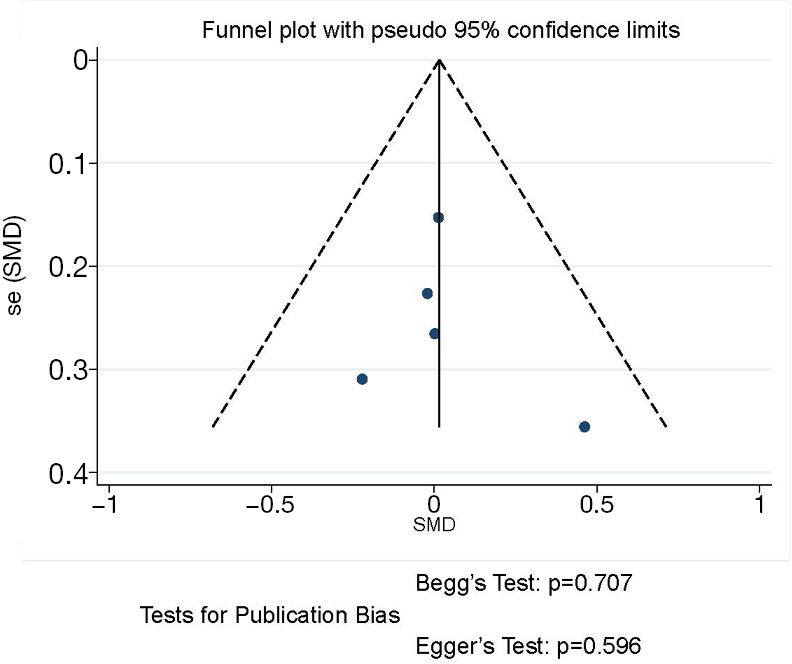
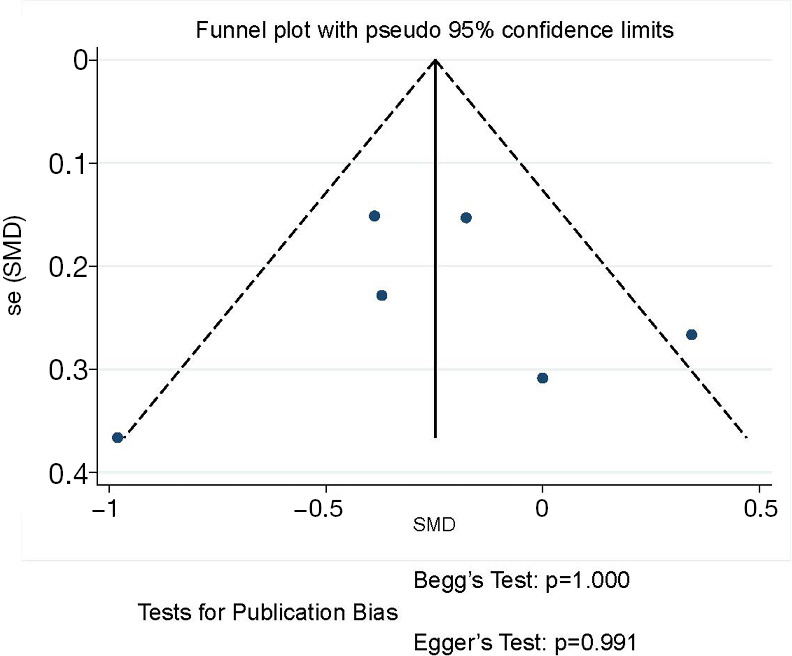
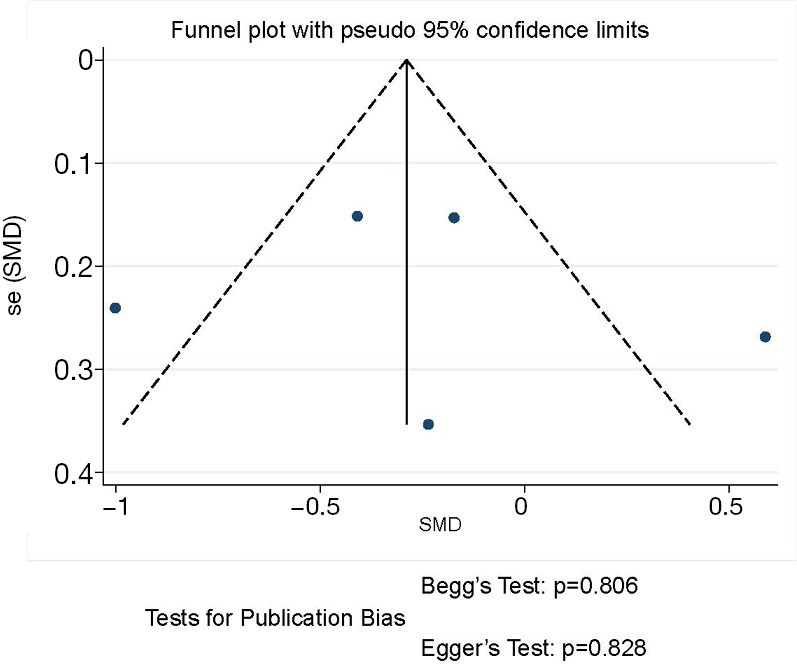
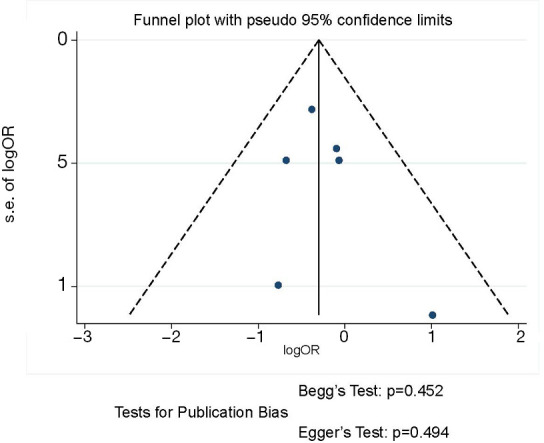
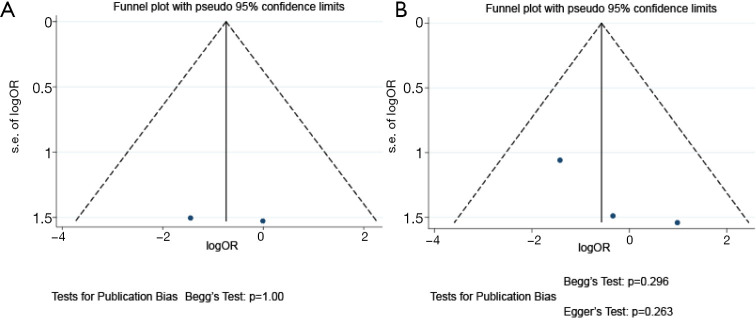
Results: Six studies generating 281 thoracoscopy and 369 thoracotomy cases were finally included. There was no significant difference in intraoperative blood loss, number of resected lymph nodes, chest drainage time, postoperative complication rate and mortality between two groups. However, thoracoscopic sleeve lobectomy was associated with longer operation time (SMD 0.59, 95% CI: 0.14 to 1.03, P=0.010). And shorter postoperative hospital stays (SMD -0.24, 95% CI: -0.51 to 0.03, P=0.078) were observed in the thoracoscopy group with marginal significance. Furthermore, sleeve lobectomy via thoracoscopy could achieve comparable OS compared to that via thoracotomy (HR 0.69, 95% CI: 0.38 to 1.00; P<0.001). In addition, there were no evident publication bias in all observational outcomes.
Conclusions: Current evidence suggests that thoracoscopic sleeve lobectomy is a safe and efficient surgical procedure for centrally located NSCLC, with comparable perioperative outcomes and equivalent oncological results compared to thoracotomy sleeve lobectomy.
Keywords: Video-assisted thoracoscopic surgery (VATS); non-small cell lung cancer (NSCLC); robotic-assisted thoracoscopic surgery (RATS); sleeve lobectomy; thoracotomy.
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/jtd-20-1855). The authors have no conflicts of interest to declare.
Figures
References
-
- Brewer LA, 3rd. The first pneumonectomy. Historical notes. J Thorac Cardiovasc Surg 1984;88:810-26. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials