

Prognostic implications of preoperative versus postoperative circulating tumor DNA in surgically resected lung cancer patients: a pilot study
- PMID: 33209612
- PMCID: PMC7653121
- DOI: 10.21037/tlcr-20-505
Prognostic implications of preoperative versus postoperative circulating tumor DNA in surgically resected lung cancer patients: a pilot study
Abstract
Background: Recent studies of advanced lung cancer patients have shown that circulating tumor DNA (ctDNA) analysis is useful for molecular profiling, monitoring tumor burden, and predicting therapeutic efficacies and disease progression. However, the usefulness of ctDNA analysis in surgically resected lung cancers is unclear.
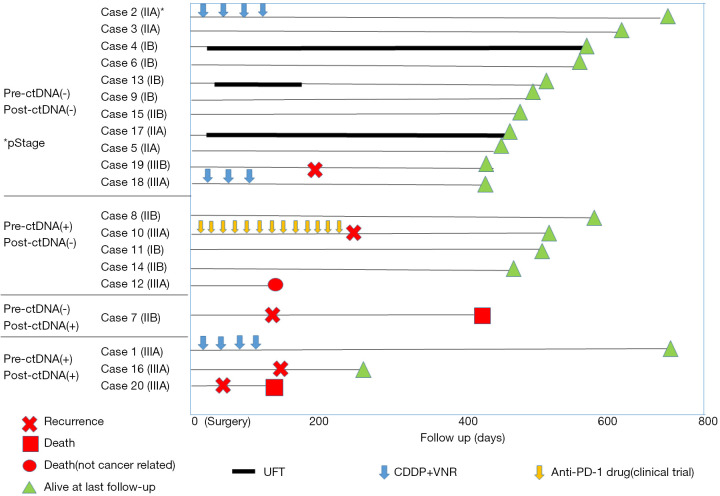
Methods: This study included 20 lung cancer patients with clinical stage IIA-IIIA disease. Preoperative and postoperative (3-12 days) plasma samples were collected for ctDNA analysis. Cancer personalized profiling by deep sequencing, which can detect mutations in 197 cancer-related genes, was used for ctDNA detection. The cohort consisted of 18 men and 2 women with a median age of 69 (range, 37-88) years. Sixteen patients (80%) had a history of smoking. Histologically, there were four squamous cell carcinomas, 13 adenocarcinomas, two adenosquamous cell carcinomas, and one small cell carcinoma.
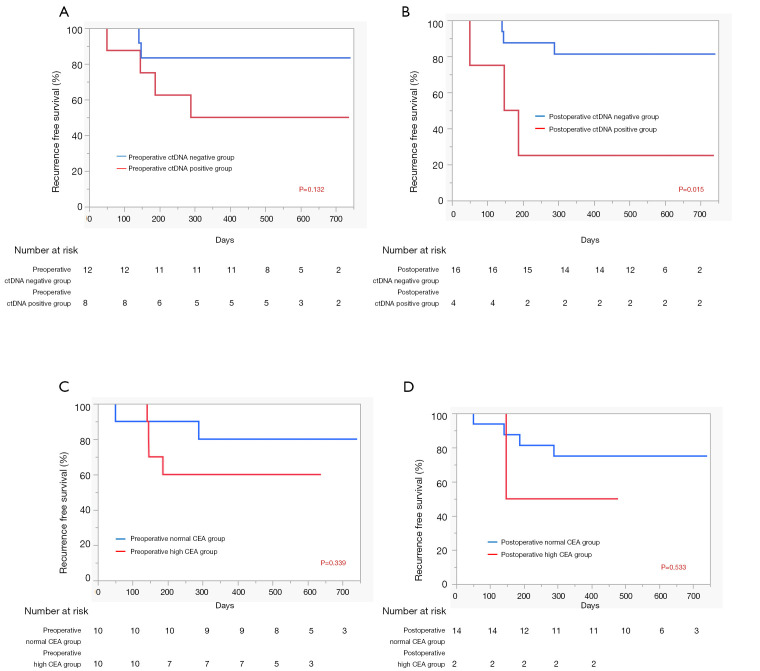
Results: At the time of data analysis, the 20 patients had been monitored for a median follow-up of 12 months. Eight patients (40%) were positive for preoperative ctDNA, and this was significantly correlated with tumor size (≥5 vs. <5 cm, P=0.018). Four patients (20%) were positive for postoperative ctDNA, and this was significantly correlated with histological grade (3 vs. 1 or 2, P=0.032). Postoperative positivity for ctDNA also predicted shorter recurrence-free survival (RFS) (P=0.015), while pre- and post-operative carcinoembryonic antigen levels (P=0.150 and P=0.533, respectively) and preoperative positivity for ctDNA (P=0.132) were not correlated with RFS.
Conclusions: Detecting ctDNA postoperatively was a poor prognostic factor in surgically resected lung cancer patients that may suggest there is minimal residual disease (MRD).
Keywords: Circulating tumor DNA (ctDNA); non-small cell lung cancer (NSCLC); prognostic factor; recurrence-free survival (RFS); surgery.
2020 Translational Lung Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/tlcr-20-505). TM serves as an unpaid editorial board member of Translational Lung Cancer Research from Sep 2019 to Sep 2021. Dr. Suda reports personal fees from AstraZeneca, grants and personal fees from Boehrinnger-Ingelheim, grants from Rain Therapeutics, outside the submitted work. Dr. Sakai reports personal fees from Roche Diagnostics, Bio-Rad, SRL Diagnostics, AstraZeneca, and Chugai Pharmaceutical, outside the submitted work. TF reports personal fees from Novartis, grants from Apollomics.Inc., outside the submitted work. KN reports grants and personal fees from Otsuka Pharmaceutical, Life Technologies Japan, Boehringer Ingelheim, and Eli Lilly; personal fees from Chugai Pharmaceutical, Eisai, from Pfizer, Novartis, MSD, Ono Pharmaceutical, Bristol-Myers Squibb, SymBio Pharmaceuticals Limited, Solasia Pharma, Yakult Honsha, Roche Diagnostics, AstraZeneca, Sanofi, Guardant Health, Takeda, and Kobayashi Pharmaceutical, grants from Ignyta, and Astellas, outside the submitted work. TM reports grants and personal fees from AstraZeneca, Boehrinnger-Ingelheim, and Pfizer, personal fees from MSD, grants and personal fees from Chugai, grants and personal fees from Ono, personal fees from Eli-Lilly, grants and personal fees from Daiiichi-Sankyo, personal fees from ThermoFisher, personal fees from Guardant, grants and personal fees from Taiho, personal fees from Amgen, and Novartis, outside the submitted work. The other authors have no conflicts of interest to declare.
Figures
References
-
- Okami J, Shintani Y, Okumura M, et al. Demographics, Safety and Quality, and Prognostic Information in Both the Seventh and Eighth Editions of the TNM Classification in 18,973 Surgical Cases of the Japanese Joint Committee of Lung Cancer Registry Database in 2010. J Thorac Oncol 2019;14:212-22. - PubMed
-
- Herbst RS, Tsuboi M, John T, et al. Osimertinib as adjuvant therapy in patients (pts) with stage IB–IIIA EGFR mutation positive (EGFRm) NSCLC after complete tumor resection: ADAURA. J Clin Oncol 2020;38:(suppl; abstr LBA5).
LinkOut - more resources
Full Text Sources