

Evaluation of the Incidence and Potential Mechanisms of Tracheal Complications in Patients With COVID-19
- PMID: 33211087
- PMCID: PMC7677875
- DOI: 10.1001/jamaoto.2020.4148
Evaluation of the Incidence and Potential Mechanisms of Tracheal Complications in Patients With COVID-19
Abstract
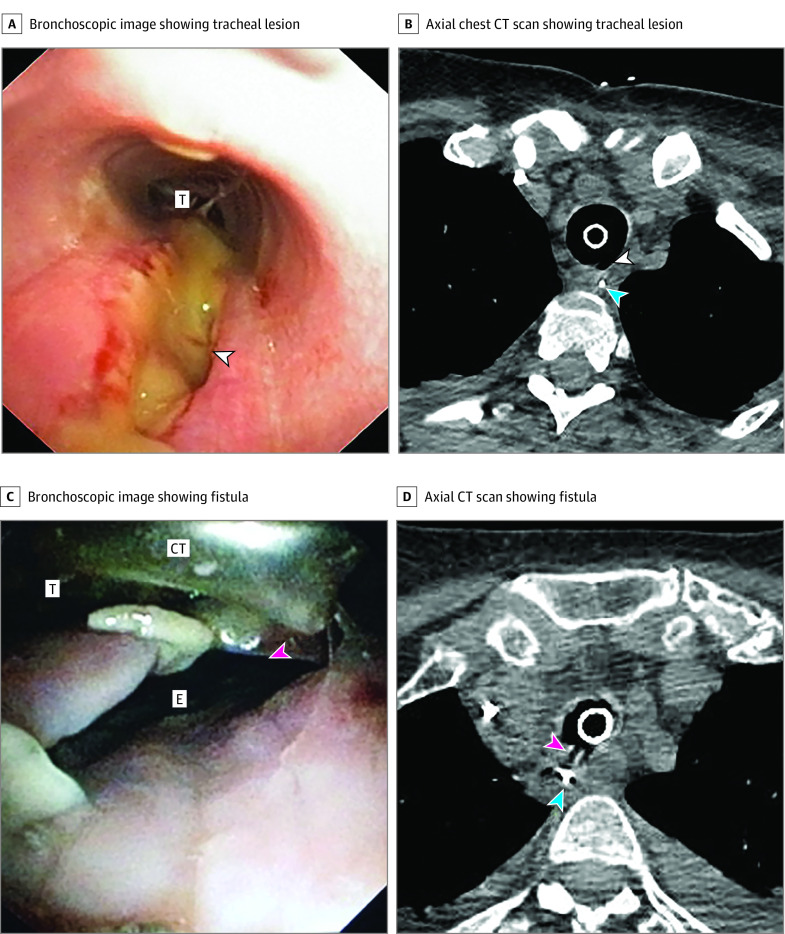
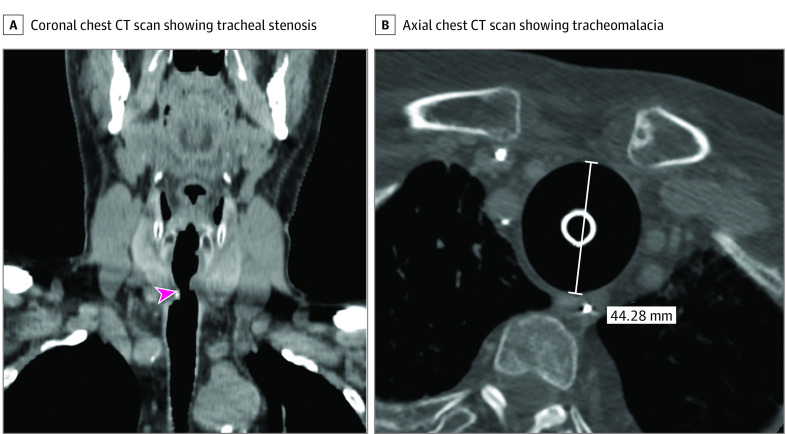
Importance: Full-thickness tracheal lesions and tracheoesophageal fistulas are severe complications of invasive mechanical ventilation. The incidence of tracheal complications in ventilated patients with coronavirus disease 2019 (COVID-19) is unknown.
Objective: To evaluate whether patients with COVID-19 have a higher incidence of full-thickness tracheal lesions and tracheoesophageal fistulas than matched controls and to investigate potential mechanisms.
Design, setting, and participants: This is a retrospective cohort study in patients admitted to the intensive care unit in a tertiary referral hospital. Among 98 consecutive patients with COVID-19 with severe respiratory failure, 30 underwent prolonged (≥14 days) invasive mechanical ventilation and were included in the COVID-19 group. The control group included 45 patients without COVID-19. Patients with COVID-19 were selected from March 1 to May 31, 2020, while the control group was selected from March 1 to May 31, 2019.
Exposures: Patients with COVID-19 had severe acute respiratory syndrome coronavirus 2 infection diagnosed by nasopharyngeal/oropharyngeal swabs and were treated according to local therapeutic procedures.
Main outcomes and measures: The primary study outcome was the incidence of full-thickness tracheal lesions or tracheoesophageal fistulas in patients with prolonged invasive mechanical ventilation.
Results: The mean (SD) age was 68.8 (9.0) years in the COVID-19 group and 68.5 (14.1) years in the control group (effect size, 0.3; 95% CI, -5.0 to 5.6). Eight (27%) and 15 (33%) women were enrolled in the COVID-19 group and the control group, respectively. Fourteen patients (47%) in the COVID-19 group had full-thickness tracheal lesions (n = 10, 33%) or tracheoesophageal fistulas (n = 4, 13%), while 1 patient (2.2%) in the control group had a full-thickness tracheal lesion (odds ratio, 38.4; 95% CI, 4.7 to 316.9). Clinical and radiological presentations of tracheal lesions were pneumomediastinum (n = 10, 71%), pneumothorax (n = 6, 43%), and/or subcutaneous emphysema (n = 13, 93%).
Conclusions and relevance: In this cohort study, almost half of patients with COVID-19 developed full-thickness tracheal lesions and/or tracheoesophageal fistulas after prolonged invasive mechanical ventilation. Attempts to prevent these lesions should be made and quickly recognized when they occur to avoid potentially life-threatening complications in ventilated patients with COVID-19.
Conflict of interest statement
Figures
Comment in
-
Laryngeal and Tracheal Pressure Injuries in Patients With COVID-19.JAMA Otolaryngol Head Neck Surg. 2021 May 1;147(5):484-485. doi: 10.1001/jamaoto.2021.0001. JAMA Otolaryngol Head Neck Surg. 2021. PMID: 33630075 No abstract available.
References
-
- Couraud L, Ballester MJ, Delaisement C. Acquired tracheoesophageal fistula and its management. Semin Thorac Cardiovasc Surg. 1996;8(4):392-399. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
