

Association Between Wearable Device-Based Measures of Physical Frailty and Major Adverse Events Following Lower Extremity Revascularization
- PMID: 33211104
- PMCID: PMC7677765
- DOI: 10.1001/jamanetworkopen.2020.20161
Association Between Wearable Device-Based Measures of Physical Frailty and Major Adverse Events Following Lower Extremity Revascularization
Abstract
Importance: Physical frailty is a key risk factor associated with higher rates of major adverse events (MAEs) after surgery. Assessing physical frailty is often challenging among patients with chronic limb-threatening ischemia (CLTI) who are often unable to perform gait-based assessments because of the presence of plantar wounds.
Objective: To test a frailty meter (FM) that does not rely on gait to determine the risk of occurrence of MAEs after revascularization for patients with CLTI.
Design, setting, and participants: This cohort study included 184 consecutively recruited patients with CLTI at 2 tertiary care centers. After 32 individuals were excluded, 152 participants were included in the study. Data collection was conducted between May 2018 and June 2019.
Exposures: Physical frailty measurement within 1 week before limb revascularization and incidence of MAEs for as long as 1 month after surgery.
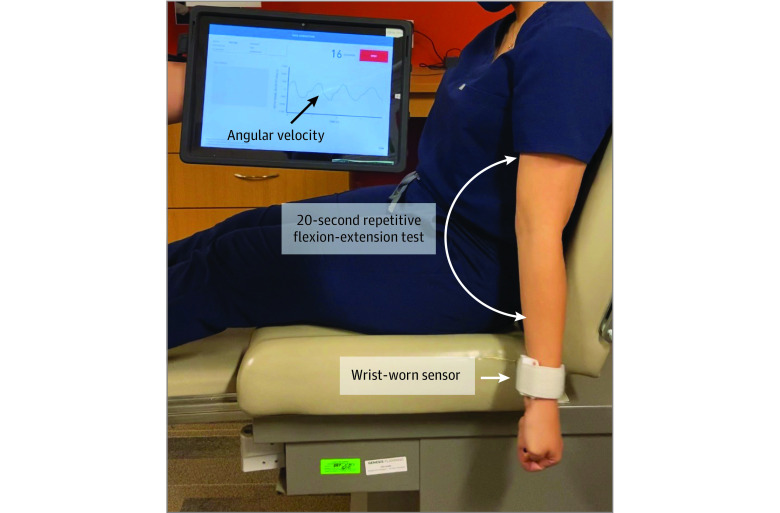
Main outcomes and measures: The FM works by quantifying weakness, slowness, rigidity, and exhaustion during a 20-second repetitive elbow flexion-extension exercise using a wrist-worn sensor. The FM generates a frailty index (FI) ranging from 0 to 1; higher values indicate progressively greater severity of physical frailty.
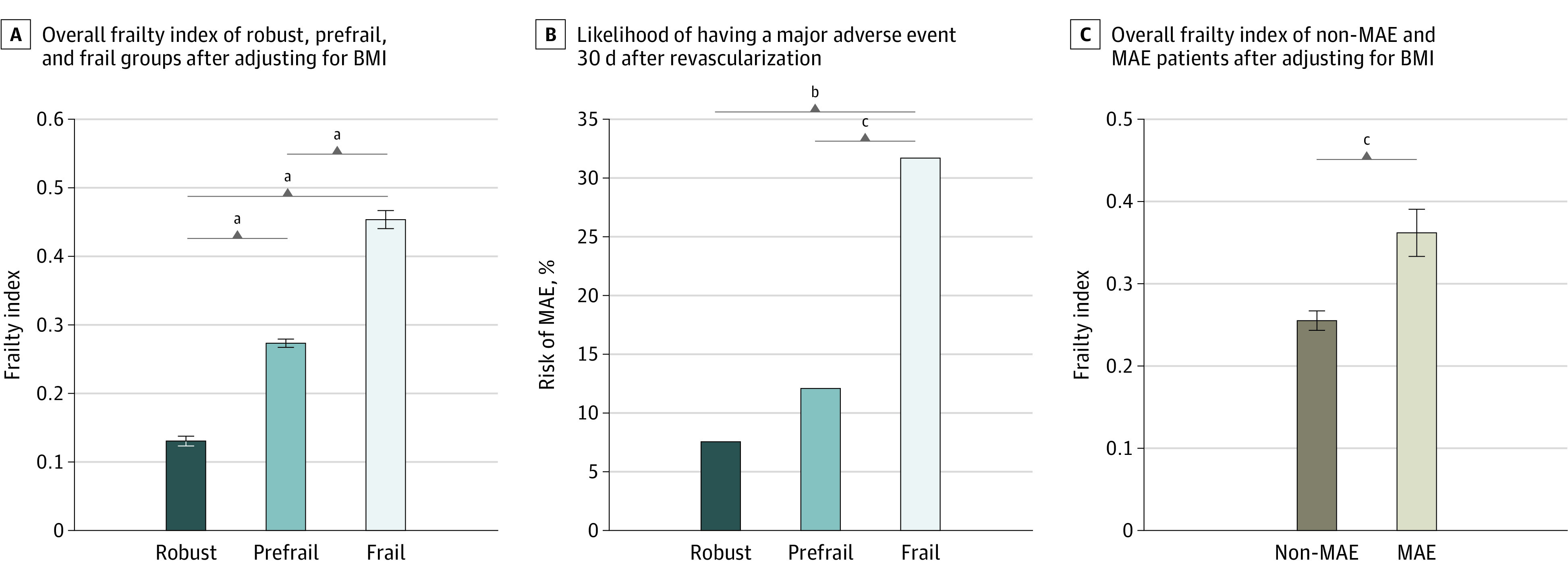
Results: Of 152 eligible participants (mean [SD] age, 67.0 [11.8] years; 59 [38.8%] women), 119 (78.2%) were unable to perform the gait test, while all could perform the FM test. Overall, 53 (34.9%), 58 (38.1%), and 41 (27.0%) were classified as robust (FI <0.20), prefrail (FI ≥0.20 to <0.35), or frail (FI ≥0.35), respectively. Within 30 days after surgery, 24 (15.7%) developed MAEs, either major adverse cardiovascular events (MACE; 8 [5.2%]) or major adverse limb events (MALE; 16 [10.5%]). Baseline demographic characteristics were not significantly different between frailty groups. In contrast, the FI was approximately 30% higher in the group that developed MAEs (mean [SD] score, 0.36 [0.14]) than those who were MAE free (mean [SD] score, 0.26 [0.13]; P = .001), with observed MAE rates of 4 patients (7.5%), 7 patients (12.1%), and 13 patients (31.7%) in the robust, prefrail and frail groups, respectively (P = .004). The FI distinguished individuals who developed MACE and MALE from those who were MAE free (MACE: mean [SD] FI score, 0.38 [0.16]; P = .03; MALE: mean [SD] FI score, 0.35 [0.13]; P = .004) after adjusting by body mass index.
Conclusions and relevance: In this cohort study, measuring physical frailty using a wrist-worn sensor during a short upper extremity test was a practical method for stratifying the risk of MAEs following revascularization for CLTI when the administration of gait-based tests is often challenging.
Conflict of interest statement
Figures
Similar articles
-
Toward Using a Smartwatch to Monitor Frailty in a Hospital Setting: Using a Single Wrist-Wearable Sensor to Assess Frailty in Bedbound Inpatients.Gerontology. 2018;64(4):389-400. doi: 10.1159/000484241. Epub 2017 Nov 25. Gerontology. 2018. PMID: 29176316 Free PMC article.
-
Sensor-Based Upper-Extremity Frailty Assessment for the Vascular Surgery Risk Stratification.J Surg Res. 2020 Feb;246:403-410. doi: 10.1016/j.jss.2019.09.029. Epub 2019 Oct 17. J Surg Res. 2020. PMID: 31630882
-
Harnessing Digital Health to Objectively Assess Functional Performance in Veterans with Chronic Obstructive Pulmonary Disease.Gerontology. 2022;68(7):829-839. doi: 10.1159/000520401. Epub 2021 Nov 29. Gerontology. 2022. PMID: 34844245 Free PMC article.
-
The frailty index based on laboratory test data as a tool to investigate the impact of frailty on health outcomes: a systematic review and meta-analysis.Age Ageing. 2023 Jan 8;52(1):afac309. doi: 10.1093/ageing/afac309. Age Ageing. 2023. PMID: 36626319 Free PMC article.
-
Development, validation and performance of laboratory frailty indices: A scoping review.Arch Gerontol Geriatr. 2023 Aug;111:104995. doi: 10.1016/j.archger.2023.104995. Epub 2023 Mar 11. Arch Gerontol Geriatr. 2023. PMID: 36963345
Cited by
-
A Wrist-Worn Sensor-Derived Frailty Index Based on an Upper-Extremity Functional Test in Predicting Functional Mobility in Older Adults.Gerontology. 2021;67(6):753-761. doi: 10.1159/000515078. Epub 2021 Apr 1. Gerontology. 2021. PMID: 33794537 Free PMC article.
-
Decoding Precision Aging: The Intersection of Cognitive Decline, Frailty, and Hormonal Biomarkers.Gerontology. 2025;71(7):564-575. doi: 10.1159/000546250. Epub 2025 May 5. Gerontology. 2025. PMID: 40359930
-
A 20-s Video-Based Assessment of Cognitive Frailty: Results from a Cohort Study within the Precision Aging Network.Gerontology. 2025;71(7):589-600. doi: 10.1159/000546227. Epub 2025 May 6. Gerontology. 2025. PMID: 40359928
-
A Remote Diet and Exercise Intervention for Surgical Patients With Prefrailty and Frailty During the COVID-19 Pandemic.Am J Lifestyle Med. 2022 May 24;17(2):176-181. doi: 10.1177/15598276221093929. eCollection 2023 Mar-Apr. Am J Lifestyle Med. 2022. PMID: 36883126 Free PMC article.
-
Cellular Senescence and Frailty in Transplantation.Curr Transplant Rep. 2023 Jun;10(2):51-59. doi: 10.1007/s40472-023-00393-6. Epub 2023 Mar 21. Curr Transplant Rep. 2023. PMID: 37576589 Free PMC article.
References
-
- Chow WB, Rosenthal RA, Merkow RP, Ko CY, Esnaola NF; American College of Surgeons National Surgical Quality Improvement Program; American Geriatrics Society . Optimal preoperative assessment of the geriatric surgical patient: a best practices guideline from the American College of Surgeons National Surgical Quality Improvement Program and the American Geriatrics Society. J Am Coll Surg. 2012;215(4):453-466. doi:10.1016/j.jamcollsurg.2012.06.017 - DOI - PubMed
