

Symptomatic Giant Primary Nonparasitic Splenic Cyst Treated with Laparoscopic Decapsulation: A Case Report and Literature Review
- PMID: 33211675
- PMCID: PMC7684427
- DOI: 10.12659/AJCR.927893
Symptomatic Giant Primary Nonparasitic Splenic Cyst Treated with Laparoscopic Decapsulation: A Case Report and Literature Review
Abstract
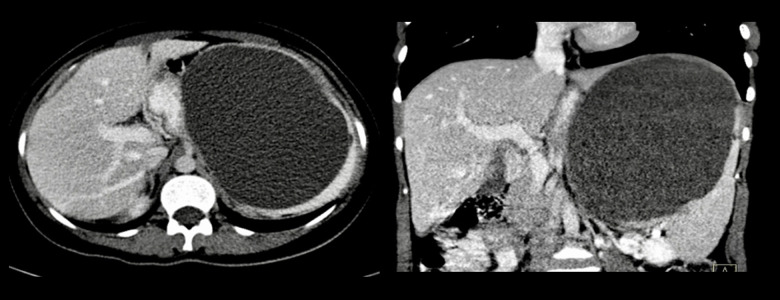
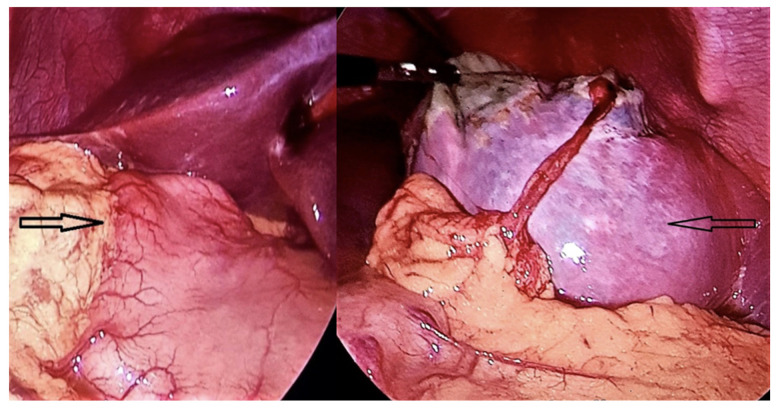
BACKGROUND Primary nonparasitic splenic cysts (PNSC) are unusual epithelial fluid lesions of the spleen. They are considered congenital cysts and are often discovered incidentally in young people. Larger cysts can be symptomatic and are traditionally managed with splenectomy. This report is of a woman with a large symptomatic PNSC that was managed surgically by laparoscopic decapsulation. CASE REPORT A 22-year-old Lebanese woman presented with left upper-quadrant pain, left pleuritic pain, food intolerance, and significant weight loss. Investigations showed a 20×17×15 cm cystic lesion in the spleen. Secondary causes were ruled out and tumor marker and hydatid serology were unremarkable. Laparoscopic decapsulation of the cyst with spleen preservation was performed with no perioperative complications. The patient's 3-year follow-up visit revealed no clinical or radiological recurrence. CONCLUSIONS True congenital splenic cysts are rare clinical findings. Generally, they do not have malignant potential. The development of minimally invasive techniques has shifted the trend toward splenic salvaging procedures. Literature review revealed an acceptable recurrence rate with near-total rather than partial unroofing. Laparoscopic decapsulation can be a safe and adequate therapeutic option in selected cases.
Conflict of interest statement
None.
Figures




References
-
- Boybeyi O, Karnak I, Tanyel FC, et al. The management of primary nonparasitic splenic cysts. Turkish J Pediatr. 2010;52:500–4. - PubMed
-
- Dachman AH, Ros PR, Murari PJ, et al. Nonparasitic splenic cysts: A report of 52 cases with radiologic-pathologic correlation. Am J Roentgenol. 1986;147(3):537–42. - PubMed
-
- Morgenstern L. Nonparasitic splenic cysts: Pathogenesis, classification, and treatment. J Am Coll Surg. 2002;194:306–14. - PubMed
-
- Safioleas M, Misiakos E, Manti C. Surgical treatment for splenic hydatidosis. World J Surg. 1997;21:374–78. - PubMed
-
- Morgenstern L. Non-parasitic splenic cysts: Pathogenesis, classification and treatment. J Am Coll Surg. 2002;194:306–14. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
