

Mode of birth and risk of infection-related hospitalisation in childhood: A population cohort study of 7.17 million births from 4 high-income countries
- PMID: 33211696
- PMCID: PMC7676705
- DOI: 10.1371/journal.pmed.1003429
Mode of birth and risk of infection-related hospitalisation in childhood: A population cohort study of 7.17 million births from 4 high-income countries
Abstract
Background: The proportion of births via cesarean section (CS) varies worldwide and in many countries exceeds WHO-recommended rates. Long-term health outcomes for children born by CS are poorly understood, but limited data suggest that CS is associated with increased infection-related hospitalisation. We investigated the relationship between mode of birth and childhood infection-related hospitalisation in high-income countries with varying CS rates.
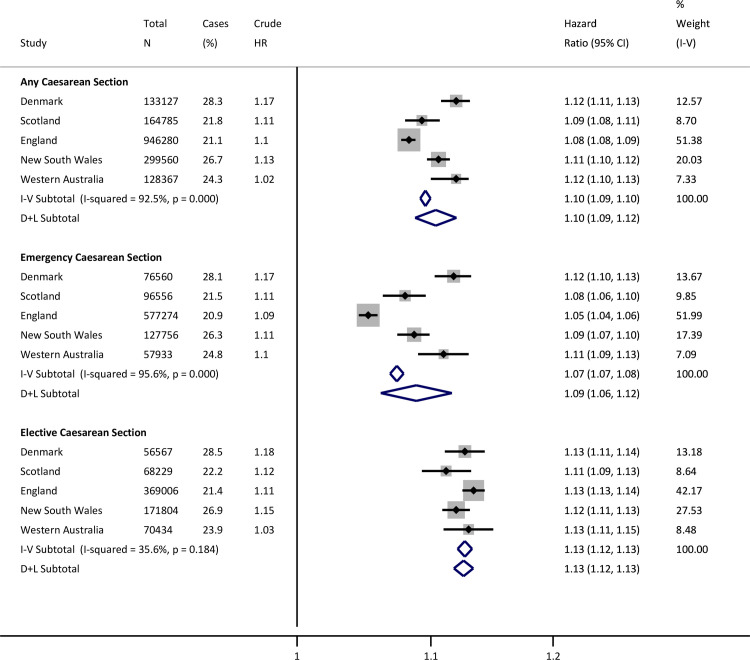
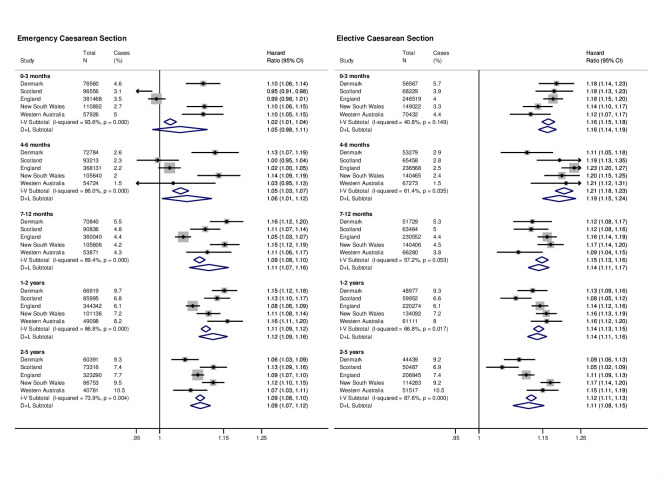
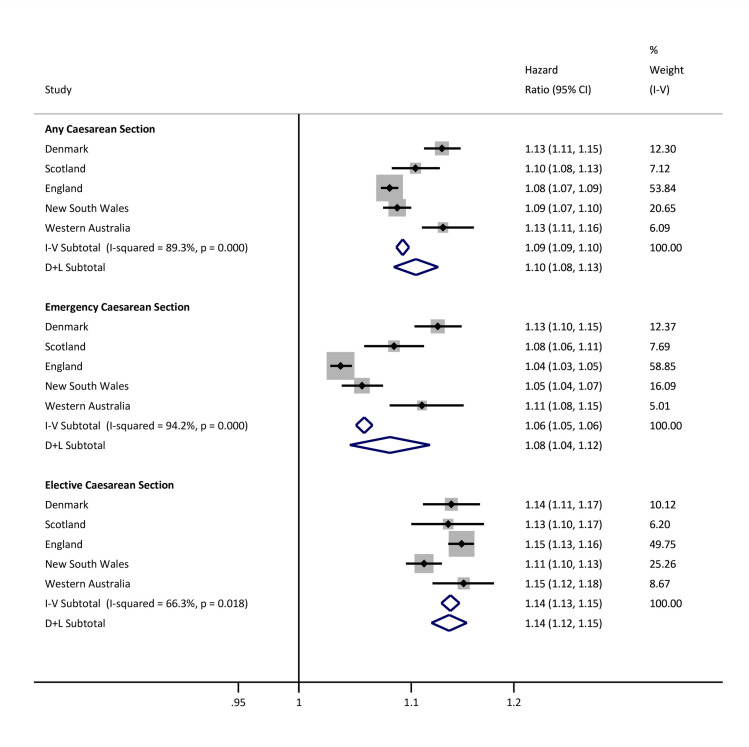
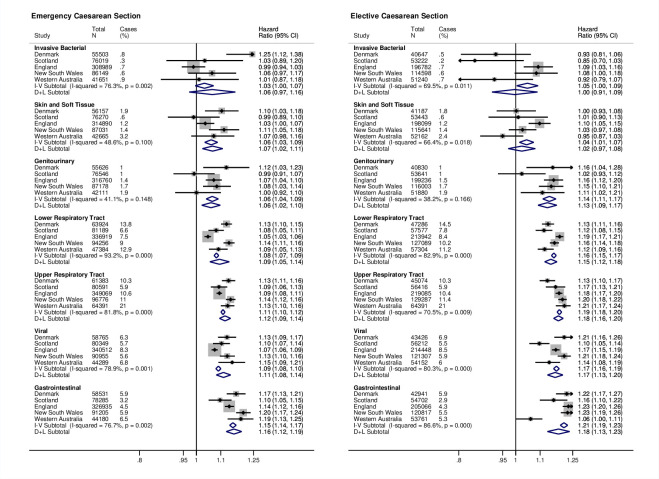
Methods and findings: We conducted a multicountry population-based cohort study of all recorded singleton live births from January 1, 1996 to December 31, 2015 using record-linked birth and hospitalisation data from Denmark, Scotland, England, and Australia (New South Wales and Western Australia). Birth years within the date range varied by site, but data were available from at least 2001 to 2010 for each site. Mode of birth was categorised as vaginal or CS (emergency/elective). Infection-related hospitalisations (overall and by clinical type) occurring after the birth-related discharge date were identified in children until 5 years of age by primary/secondary International Classification of Diseases, 10th Revision (ICD-10) diagnosis codes. Analysis used Cox regression models, adjusting for maternal factors, birth parameters, and socioeconomic status, with results pooled using meta-analysis. In total, 7,174,787 live recorded births were included. Of these, 1,681,966 (23%, range by jurisdiction 17%-29%) were by CS, of which 727,755 (43%, range 38%-57%) were elective. A total of 1,502,537 offspring (21%) had at least 1 infection-related hospitalisation. Compared to vaginally born children, risk of infection was greater among CS-born children (hazard ratio (HR) from random effects model, HR 1.10, 95% confidence interval (CI) 1.09-1.12, p < 0.001). The risk was higher following both elective (HR 1.13, 95% CI 1.12-1.13, p < 0.001) and emergency CS (HR 1.09, 95% CI 1.06-1.12, p < 0.001). Increased risks persisted to 5 years and were highest for respiratory, gastrointestinal, and viral infections. Findings were comparable in prespecified subanalyses of children born to mothers at low obstetric risk and unchanged in sensitivity analyses. Limitations include site-specific and longitudinal variations in clinical practice and in the definition and availability of some data. Data on postnatal factors were not available.
Conclusions: In this study, we observed a consistent association between birth by CS and infection-related hospitalisation in early childhood. Notwithstanding the limitations of observational data, the associations may reflect differences in early microbial exposure by mode of birth, which should be investigated by mechanistic studies. If our findings are confirmed, they could inform efforts to reduce elective CS rates that are not clinically indicated.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Comment in
-
Cesarean section and childhood infections: Causality for concern?PLoS Med. 2020 Nov 19;17(11):e1003457. doi: 10.1371/journal.pmed.1003457. eCollection 2020 Nov. PLoS Med. 2020. PMID: 33211689 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
